
Pulmonary Rehabilitation Programmes: Structure, Evidence and Outcomes
Learn the components, duration, outcome measures and evidence for pulmonary rehabilitation in COPD, ILD and other chronic lung diseases.
Pulmonary rehabilitation is a comprehensive, individualised programme combining exercise, education and behaviour-change strategies to improve the physical and psychological well-being of people with chronic respiratory disease.
Pulmonary rehabilitation is often misunderstood as a short course of breathing exercises. In reality, it is a comprehensive, individualised intervention that combines exercise training, education and behaviour change following a detailed patient assessment. Its purpose is not to reverse the underlying lung pathology but to reduce symptoms, improve functional capacity and help people manage chronic respiratory disease more independently (Rochester et al., 2023; Spruit et al., 2013).
This distinction is important in examinations and clinical practice: pulmonary rehabilitation primarily improves how the patient functions, rather than substantially changing spirometry.
Who Should Be Referred for Pulmonary Rehabilitation?
Pulmonary rehabilitation should be considered when chronic respiratory disease causes breathlessness, exercise limitation, reduced participation in daily activities or repeated healthcare use despite appropriate medical management.
In COPD, current recommendations support referral for patients with relevant symptoms or increased exacerbation risk, including after hospitalisation for an acute exacerbation. Referral should not depend on FEV₁ alone because exercise intolerance may be influenced by peripheral muscle dysfunction, dynamic hyperinflation, anxiety, nutritional problems and comorbidities as much as by airflow obstruction (Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026).
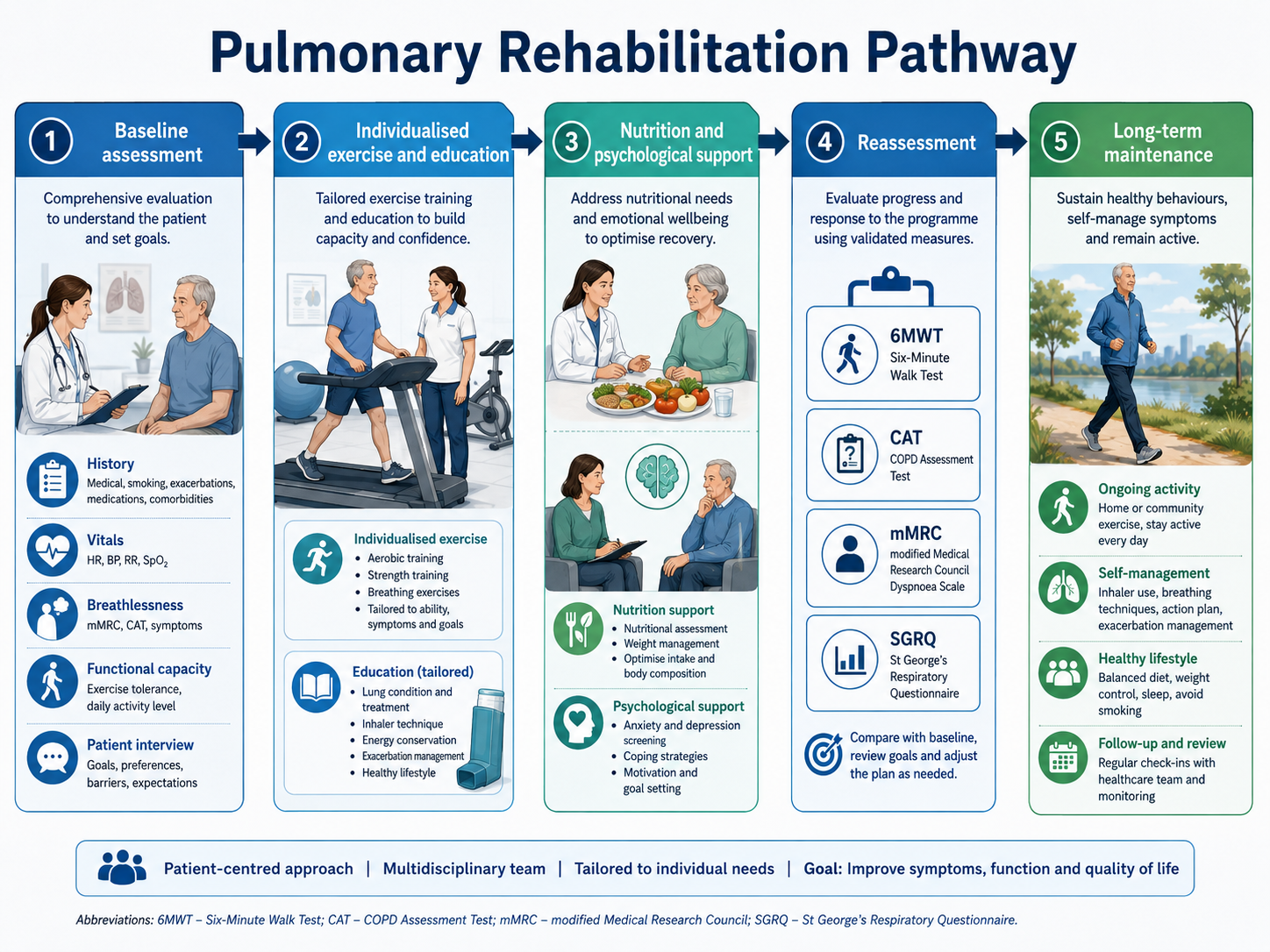
Before exercise begins, the multidisciplinary team assesses medical stability, symptoms, functional capacity, oxygenation, comorbidities, falls risk, nutritional status and psychological health. Baseline measures are then repeated at programme completion to determine whether meaningful improvement has occurred.
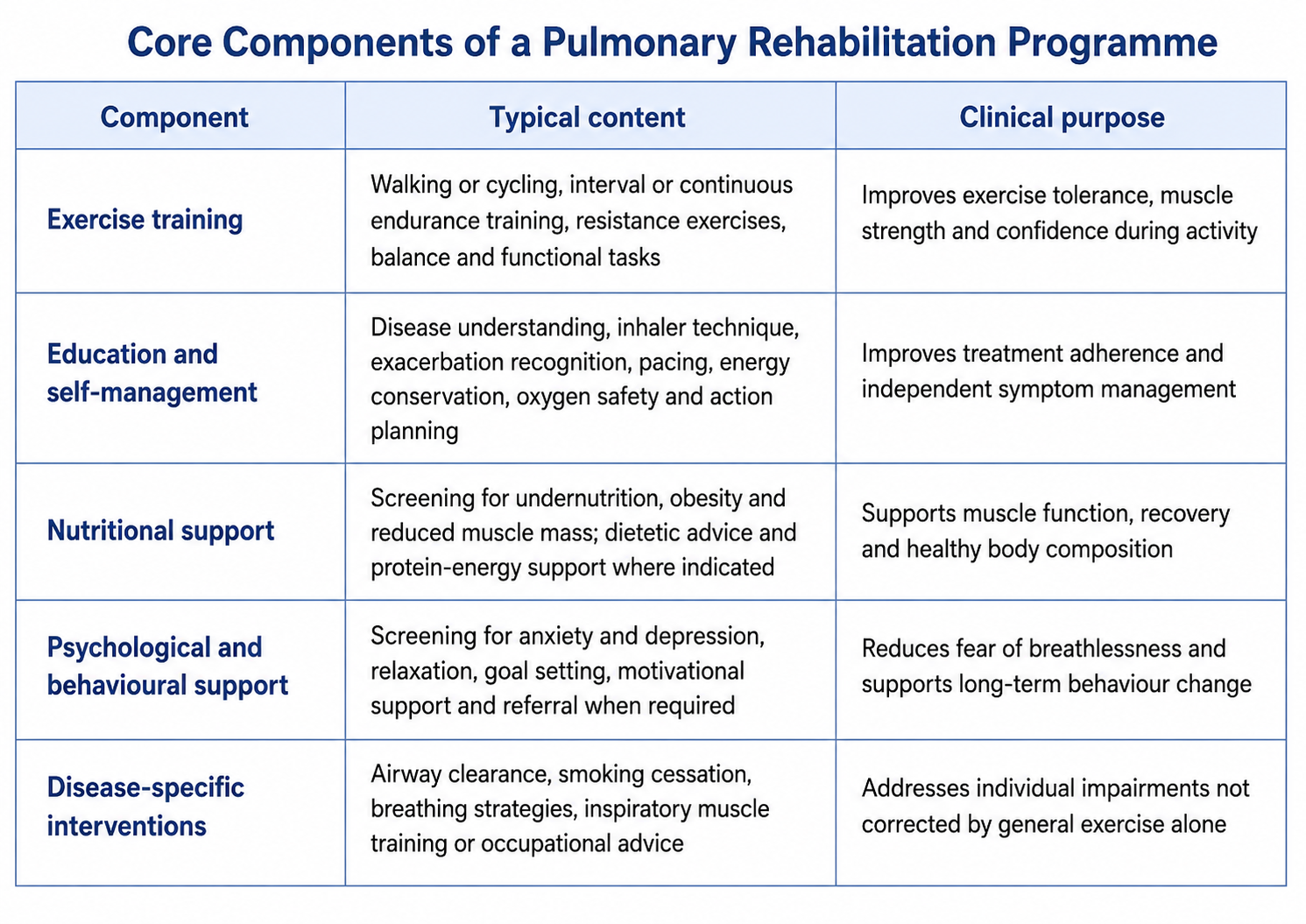
Core Components of a Pulmonary Rehabilitation Programme
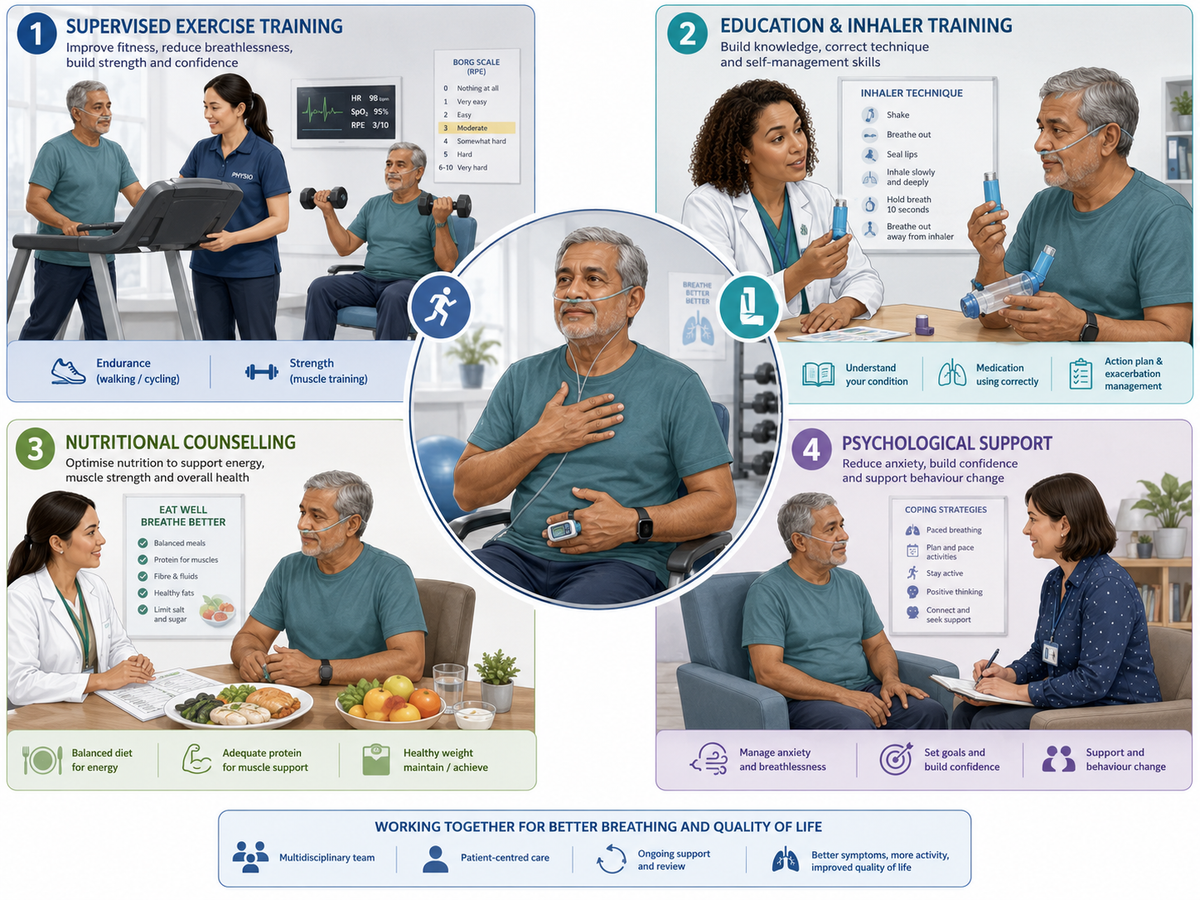
Exercise training is the central component, but exercise alone does not constitute comprehensive pulmonary rehabilitation. Traditional physiotherapy texts and modern guidelines emphasise an integrated approach addressing physical, behavioural and psychosocial limitations (Downie, 1993; Frownfelter et al., 2022; Hillegass, 2022).
Exercise training
Aerobic training commonly uses walking or cycling and may be prescribed continuously or as intervals. Interval training is particularly useful when severe dyspnoea, fatigue or desaturation prevents sustained exercise. Resistance training targets major upper- and lower-limb muscle groups and is important because limb muscle weakness contributes directly to activity limitation.
Training intensity is progressed according to symptoms, heart rate, oxygen saturation, workload and perceived exertion. Supplemental oxygen may be required for selected patients with clinically significant exercise-induced desaturation. Inspiratory muscle training can be added when inspiratory muscle weakness is documented, but it should not replace whole-body exercise.
Education, nutrition and psychological care
Education should lead to behaviour change rather than simply provide information. Patients practise inhaler use, symptom monitoring, pacing and decision-making for exacerbations. Nutritional management must also be individualised. Some patients have obesity and increased ventilatory demand, while others develop low body mass or reduced fat-free mass. Both patterns can worsen exercise tolerance. Anxiety, depression and fear of breathlessness may reinforce inactivity. Psychological support, graded exposure to activity and achievable goal setting help interrupt the cycle of breathlessness, avoidance, deconditioning and further breathlessness.
Eight-Week Versus Twelve-Week Programmes
Most outpatient programmes last approximately 6–12 weeks, with 8-week and 12-week formats commonly used. The optimal duration is not determined by the calendar alone; total exercise exposure, progression, attendance and adherence to home training are equally important.
An 8-week programme is practical, less resource-intensive and capable of producing clinically meaningful improvements when exercise is appropriately prescribed and progressed. A 12-week programme provides additional time for patients with severe deconditioning, multiple comorbidities, low exercise confidence or slower progression.
The PuRe Duration Trial directly compared twice-weekly supervised 8-week and 12-week programmes in COPD. Improvements in endurance exercise capacity were broadly equivalent, although some findings suggested that longer participation might provide additional benefit for selected functional and health-related quality-of-life outcomes (Bishop et al., 2025).
Therefore, 12 weeks should not automatically be considered superior for every patient. An effective 8-week programme is preferable to a poorly attended 12-week course. Conversely, rigidly discharging a patient at eight weeks may be inappropriate when further supervised progression is clinically justified.
After either format, patients require a maintenance plan involving independent exercise, community activity, periodic review or a supervised maintenance programme. Without continued physical activity, some benefits decline over time.
Outcome Measures: What Should Be Reassessed?
Pulmonary rehabilitation outcomes should extend beyond spirometry. Lung function may remain relatively unchanged even when the patient can walk farther, perform daily activities more easily and experience less breathlessness.
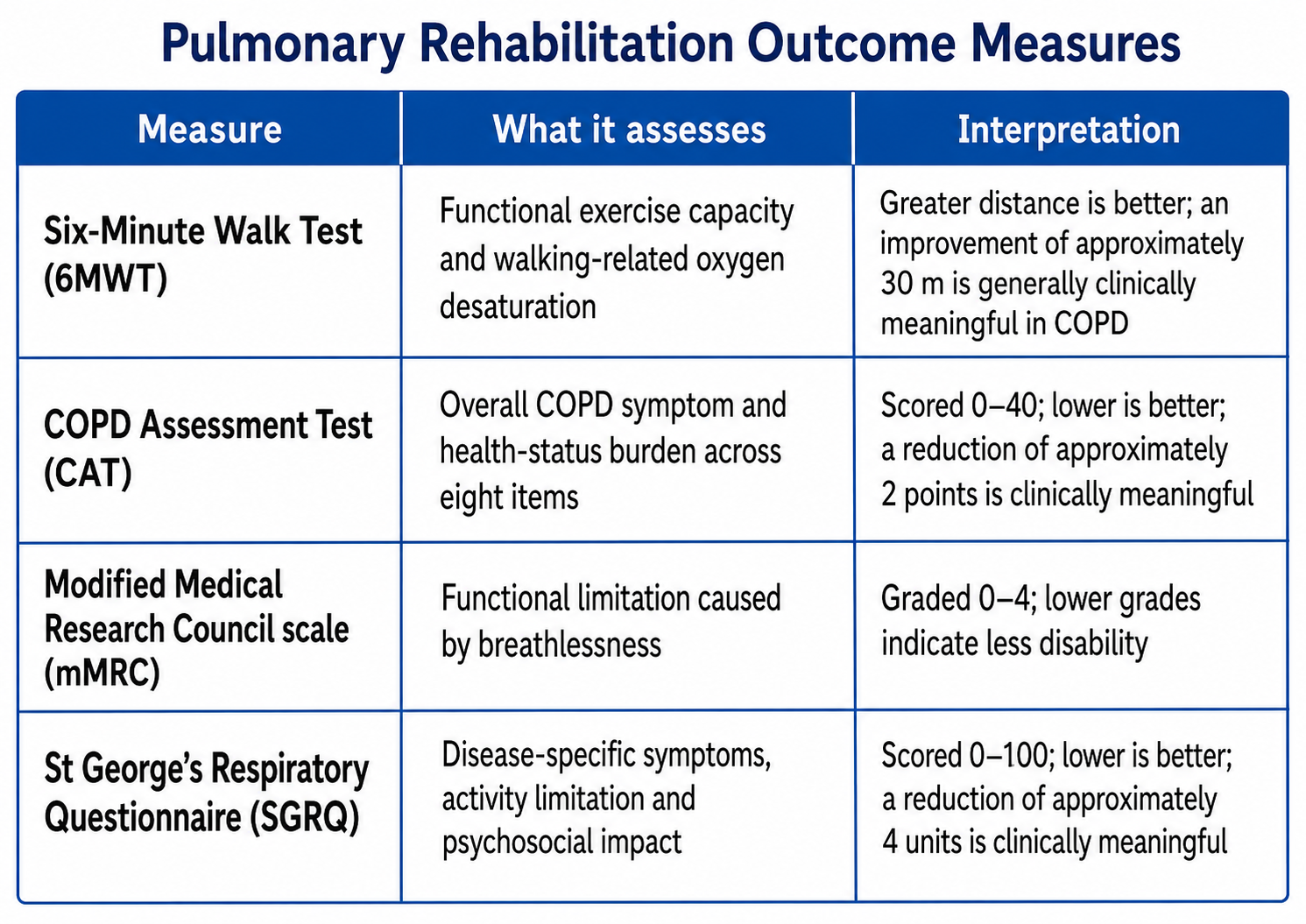
The 6MWT should be performed using a standardised protocol and comparable oxygen, walking-aid and encouragement conditions at reassessment. Pulse rate, oxygen saturation and Borg breathlessness or exertion scores provide additional information beyond distance.
The CAT is brief and practical for routine COPD care, whereas the SGRQ provides a more detailed evaluation of respiratory health status. The mMRC is useful for rapid grading but is comparatively broad and should not be the sole measure of rehabilitation response (Jones, 2005; Kon et al., 2014; Polkey et al., 2013).
Programme evaluation may also include quadriceps strength, sit-to-stand tests, anxiety and depression scales, physical activity, exacerbations, hospital admissions, return to work and patient-defined goals.
How Strong Is the Evidence?
COPD: the strongest evidence base
COPD has the largest and most consistent evidence base. Pulmonary rehabilitation improves exercise capacity, dyspnoea and health-related quality of life across a range of disease severities (McCarthy et al., 2015). GOLD 2026 classifies the evidence for improved dyspnoea, exercise tolerance and health status in stable COPD as high level.
The ATS provides strong recommendations, based on moderate-quality evidence, for pulmonary rehabilitation in both stable COPD and following hospitalisation for an exacerbation (Rochester et al., 2023). Post-exacerbation rehabilitation can also reduce subsequent hospitalisation, although timing, patient stability and programme uptake remain important.
Interstitial lung disease
Pulmonary rehabilitation improves exercise capacity, breathlessness and quality of life in interstitial lung disease, including idiopathic pulmonary fibrosis. The ATS recommendation is strong with moderate-quality evidence, although benefits may decline after programme completion and do not establish improved survival (Dowman et al., 2021; Rochester et al., 2023). Patients with ILD may desaturate rapidly during exercise. Oxygen assessment, interval training and closer saturation monitoring are therefore particularly important.
Pulmonary hypertension
Exercise-based rehabilitation can improve functional capacity and quality of life in pulmonary hypertension, but the evidence is less certain. The ATS recommendation is conditional and based on low-quality evidence. Patients should be medically stable and exercise under appropriately trained supervision because syncope, right-heart dysfunction and haemodynamic instability require specialist precautions.
Bronchiectasis, asthma and other conditions
In bronchiectasis, smaller studies support improvements in exercise capacity and quality of life. Programmes should incorporate airway-clearance review and infection-control procedures.
Exercise-based rehabilitation may also benefit selected patients with severe asthma, lung cancer, post-transplant limitations or persistent post-COVID respiratory disability. However, the studies are fewer and more heterogeneous than in COPD. Disease-specific adaptations are therefore essential, and the strength of evidence should not be presented as equivalent across all respiratory diagnoses (Evans, 2024).
Viva-Ready Summary
- Pulmonary rehabilitation is a multidisciplinary, patient-tailored intervention, not merely a set of breathing exercises.
- Its core components are exercise training, education and self-management, nutritional care and psychological or behavioural support.
- Eight-week and 12-week programmes can both be effective; programme quality, training dose and adherence matter more than duration alone.
- The 6MWT, CAT, mMRC and SGRQ measure different but complementary aspects of rehabilitation response.
- Evidence is strongest for COPD, strong but smaller for ILD, conditional for pulmonary hypertension and promising but less extensive for bronchiectasis and other respiratory diseases.
- Successful discharge requires a long-term maintenance and physical-activity plan.
One-line recall point: Pulmonary rehabilitation improves the patient’s capacity, symptoms and participation—even when lung function itself changes very little.
References
Bishop, J. A., Spencer, L. M., Dwyer, T. J., McKeough, Z. J., McAnulty, A., Leung, R., & Alison, J. A. (2025). Effect of pulmonary rehabilitation duration on exercise capacity and health-related quality of life in people with chronic obstructive pulmonary disease: The PuRe Duration Trial. Respirology, 30(1), 41–50. doi:10.1111/resp.14820
Downie, P. A. (Ed.). (1993). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Jaypee Brothers.
Dowman, L., Hill, C. J., May, A., & Holland, A. E. (2021). Pulmonary rehabilitation for interstitial lung disease. Cochrane Database of Systematic Reviews, (2), CD006322. doi:10.1002/14651858.CD006322.pub4
Evans, R. A. (2024). The rationale, evidence, and adaptations to pulmonary rehabilitation for chronic respiratory diseases other than COPD. Respiratory Care, 69(6), 697–712. doi:10.4187/respcare.12089
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for the prevention, diagnosis and management of chronic obstructive pulmonary disease: 2026 report.
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Jones, P. W. (2005). St. George’s Respiratory Questionnaire: MCID. COPD: Journal of Chronic Obstructive Pulmonary Disease, 2(1), 75–79.
Kon, S. S. C., Canavan, J. L., Jones, S. E., Nolan, C. M., Clark, A. L., Dickson, M. J., Haselden, B. M., Polkey, M. I., & Man, W. D.-C. (2014). Minimum clinically important difference for the COPD Assessment Test: A prospective analysis. The Lancet Respiratory Medicine, 2(3), 195–203.
McCarthy, B., Casey, D., Devane, D., Murphy, K., Murphy, E., & Lacasse, Y. (2015). Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews, (2), CD003793. doi:10.1002/14651858.CD003793.pub3
Polkey, M. I., Spruit, M. A., Edwards, L. D., Watkins, M. L., Pinto-Plata, V., Vestbo, J., Calverley, P. M. A., Tal-Singer, R., Agustí, A., Bakke, P. S., Coxson, H. O., Lomas, D. A., MacNee, W., Rennard, S., Silverman, E. K., Miller, B. E., Crim, C., Yates, J., Wouters, E. F. M., & Celli, B. (2013). Six-minute-walk test in chronic obstructive pulmonary disease: Minimal clinically important difference for death or hospitalization. American Journal of Respiratory and Critical Care Medicine, 187(4), 382–386.
Rochester, C. L., Alison, J. A., Carlin, B., Jenkins, A. R., Cox, N. S., Bauldoff, G., Bhatt, S. P., Bourbeau, J., Burtin, C., Camp, P. G., Cascino, T. M., Dorney Koppel, G. A., Garvey, C., Goldstein, R., Harris, D., Houchen-Wolloff, L., Limberg, T., Lindenauer, P. K., Moy, M. L., … Holland, A. E. (2023). Pulmonary rehabilitation for adults with chronic respiratory disease: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 208(4), e7–e26. doi:10.1164/rccm.202306-1066ST
Spruit, M. A., Singh, S. J., Garvey, C., ZuWallack, R., Nici, L., Rochester, C., Hill, K., Holland, A. E., Lareau, S. C., Man, W. D.-C., Pitta, F., Sewell, L., Raskin, J., Bourbeau, J., Crouch, R., Franssen, F. M. E., Casaburi, R., Vercoulen, J. H., Vogiatzis, I., … Wouters, E. F. M. (2013). An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine, 188(8), e13–e64. doi:10.1164/rccm.201309-1634ST



