
Post-CABG Complications: What Physios Must Screen
Learn how physiotherapists identify and manage atelectasis, postoperative atrial fibrillation and brachial plexopathy after CABG, including the causes of left-lower-lobe atelectasis.
Coronary artery bypass grafting improves myocardial perfusion, but the early postoperative period remains vulnerable to respiratory, cardiovascular and neurological complications. Physiotherapists are often among the first professionals to observe the patient during upright positioning, breathing exercises and mobilisation. A subtle fall in oxygen saturation, an unexpectedly irregular pulse or new hand weakness may therefore first become apparent during a physiotherapy session.
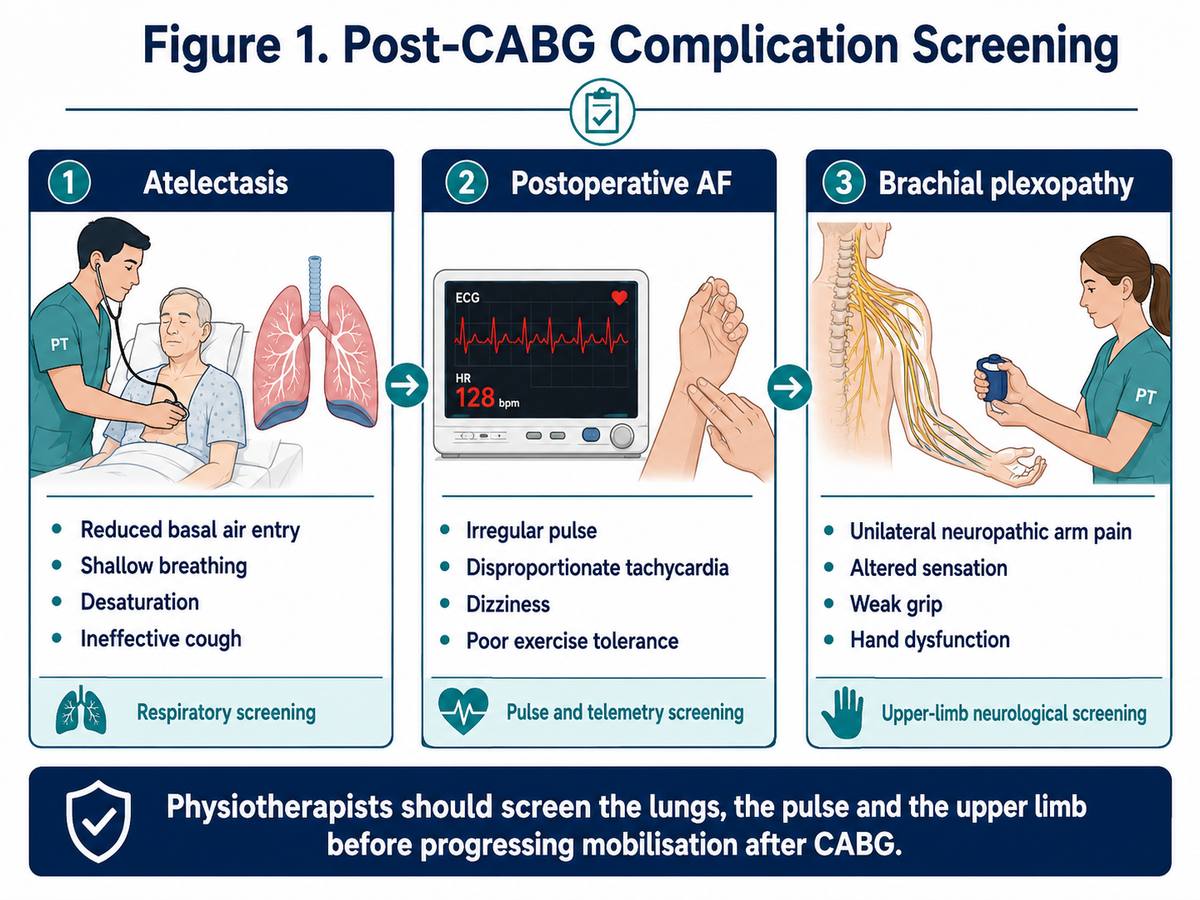
Three complications deserve particular attention: atelectasis, postoperative atrial fibrillation and brachial plexopathy. Their severity and frequency differ, but each can delay mobilisation and functional recovery. The physiotherapist’s responsibility is not to provide definitive medical treatment; it is to recognise the pattern, modify or stop treatment when necessary, and escalate concerns promptly.
Why Complication Screening Must Precede Mobilisation
Before every post-CABG session, the physiotherapist should review the operative notes, graft harvest details, chest radiograph, oxygen requirement, haemoglobin, telemetry and current medications. Baseline respiratory rate, oxygen saturation, pulse rhythm, blood pressure, pain, consciousness and perceived effort should then be documented.
Assessment must remain continuous during activity. A patient who appears stable in bed may develop exertional desaturation, a rapid irregular rhythm or neurological symptoms once sitting or walking. Enhanced recovery pathways support early mobilisation, but only after the patient has demonstrated adequate respiratory, cardiovascular and neurological stability (Grant et al., 2024).
Atelectasis: The Most Common Pulmonary Finding
Atelectasis is incomplete expansion or collapse of alveoli. It appears on approximately 30%–72% of postoperative chest radiographs following cardiac surgery, although radiological atelectasis does not always produce clinically significant respiratory dysfunction (Tanner & Colvin, 2020).
Its mechanism is multifactorial. General anaesthesia, mechanical ventilation and cardiopulmonary bypass reduce functional residual capacity and alter surfactant function. Median sternotomy, chest drains and incisional pain encourage rapid, shallow breathing, while prolonged supine positioning preferentially reduces ventilation in dependent basal segments. Diaphragmatic dysfunction, retained secretions and weak coughing may further obstruct peripheral airways.
On assessment, the patient may demonstrate reduced basal chest expansion, diminished breath sounds, fine inspiratory crackles, tachypnoea, an ineffective cough or an increased oxygen requirement. Oxygen saturation may fall during repositioning or walking. Chest radiography may show plate-like basal opacities, volume loss or elevation of a hemidiaphragm. Fever and leucocytosis during the first postoperative days are not sufficient to diagnose pneumonia because both may reflect the normal inflammatory response to surgery.
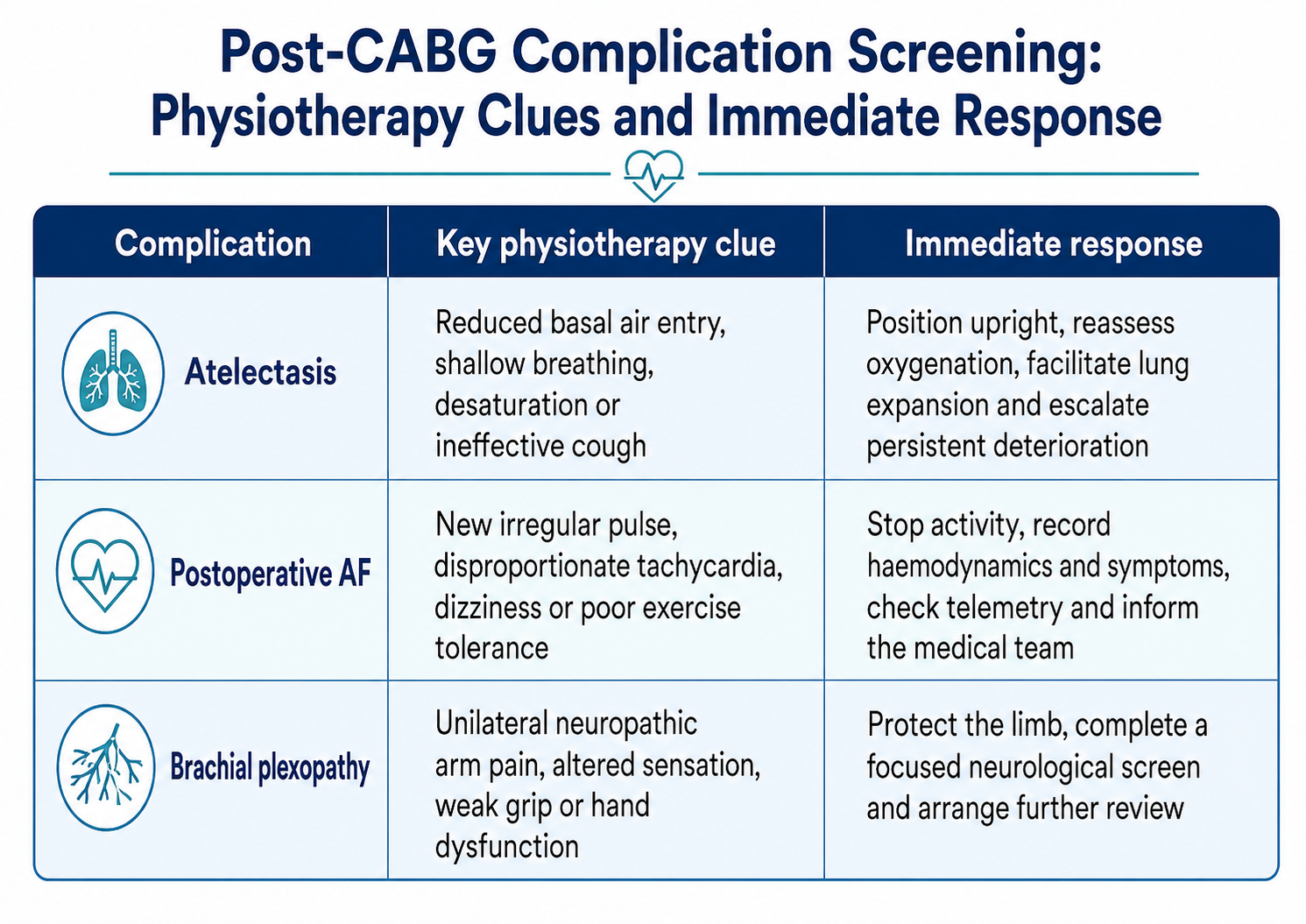
The physiotherapy approach begins with pain-aware positioning. Upright sitting, frequent position changes and early mobilisation improve dependent lung ventilation. Slow deep inspirations with a brief inspiratory hold, thoracic expansion exercises and supported huffing or coughing may be prescribed according to the patient’s capacity. Airway-clearance techniques should be targeted to patients with retained secretions rather than applied routinely to every patient. Incentive spirometry may support visual feedback, but it should not replace supervised breathing practice and mobilisation. Deep-breathing exercises have been shown to reduce atelectatic areas and improve pulmonary function following CABG (Westerdahl et al., 2005).
Persistent desaturation, increasing respiratory distress, inability to clear secretions, suspected mucus plugging or failure to improve requires medical reassessment. The multidisciplinary team may consider lung ultrasound, repeat imaging, non-invasive ventilatory support or bronchoscopy depending on the cause.
Viva Focus: Why Is Left-Lower-Lobe Atelectasis Common After CABG?
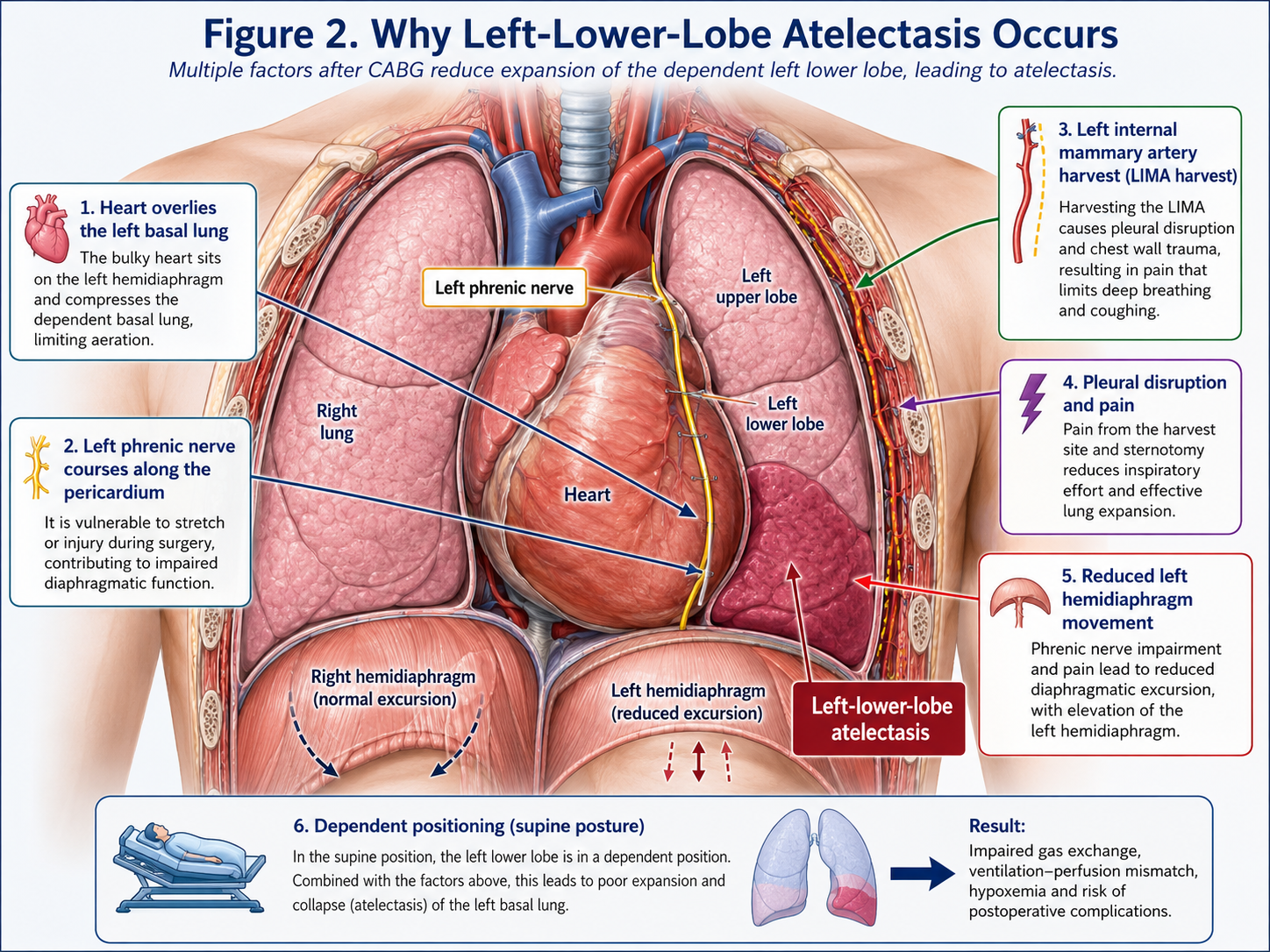
The left lower lobe is particularly vulnerable because it lies in a dependent position beneath the heart and may expand poorly when the patient remains supine. Harvesting the left internal mammary artery may require opening or manipulating the left pleura, further altering local ventilation and causing pain around the left chest drain.
A classic explanation involves the left phrenic nerve. During traditional cardiac surgery, topical ice or cold slush was placed around the heart for myocardial protection. Because the left phrenic nerve runs along the pericardium, cooling could cause temporary neuropraxia, left hemidiaphragmatic paresis and subsequent left basal collapse. Older studies demonstrated a strong relationship between topical cooling, left diaphragmatic dysfunction and left-lower-lobe atelectasis (Benjamin et al., 1982). Modern myocardial-protection techniques have reduced this risk, but the mechanism remains an important viva topic.
The key examination point is that left-lower-lobe atelectasis is multifactorial, not simply proof of phrenic nerve injury. Pain, pleural disruption, reduced diaphragmatic excursion, prolonged recumbency and secretion retention frequently coexist. A raised left hemidiaphragm, paradoxical abdominal movement, unexplained orthopnoea or persistent left basal volume loss should prompt assessment for diaphragmatic dysfunction.
Postoperative Atrial Fibrillation: Recognising an Unstable Rhythm
Postoperative atrial fibrillation is the most frequent arrhythmia after cardiac surgery. It occurs in approximately 10%–40% of patients after isolated CABG and most commonly begins around postoperative days two to four (Suero et al., 2024).
Surgical inflammation, atrial manipulation, oxidative stress, heightened sympathetic activity and pre-existing atrial fibrosis create an electrically unstable atrial substrate. Fluid shifts, electrolyte abnormalities, atrial stretch, myocardial ischaemia and interruption of beta-blockers may provide additional triggers. Older age, previous AF, left atrial enlargement, reduced ventricular function, renal disease and chronic lung disease increase susceptibility.
The physiotherapist may first detect an irregularly irregular pulse, an unexpectedly high heart rate or poor heart-rate recovery after activity. Patients may report palpitations, breathlessness, chest discomfort, dizziness, marked fatigue or reduced exercise tolerance, although some episodes are asymptomatic and identified only on telemetry.
A new or unassessed irregular rhythm should not be treated as a normal exercise response. Activity should be stopped or deferred while the patient is positioned safely and pulse, blood pressure, oxygen saturation, symptoms and telemetry are reviewed. Chest pain, hypotension, altered consciousness, syncope, acute pulmonary oedema or severe breathlessness require immediate escalation.
Rate control, rhythm control and anticoagulation decisions are medically led. Once the rhythm is medically assessed and the patient is haemodynamically stable, low-intensity mobilisation may resume with clearance. Rating of perceived exertion, symptoms and blood pressure are especially important because heart rate may be unreliable during AF and further modified by beta-blockers. Exercise progression should be conservative until the ventricular response and clinical condition are stable.
Brachial Plexopathy: The Easily Missed Neurological Complication
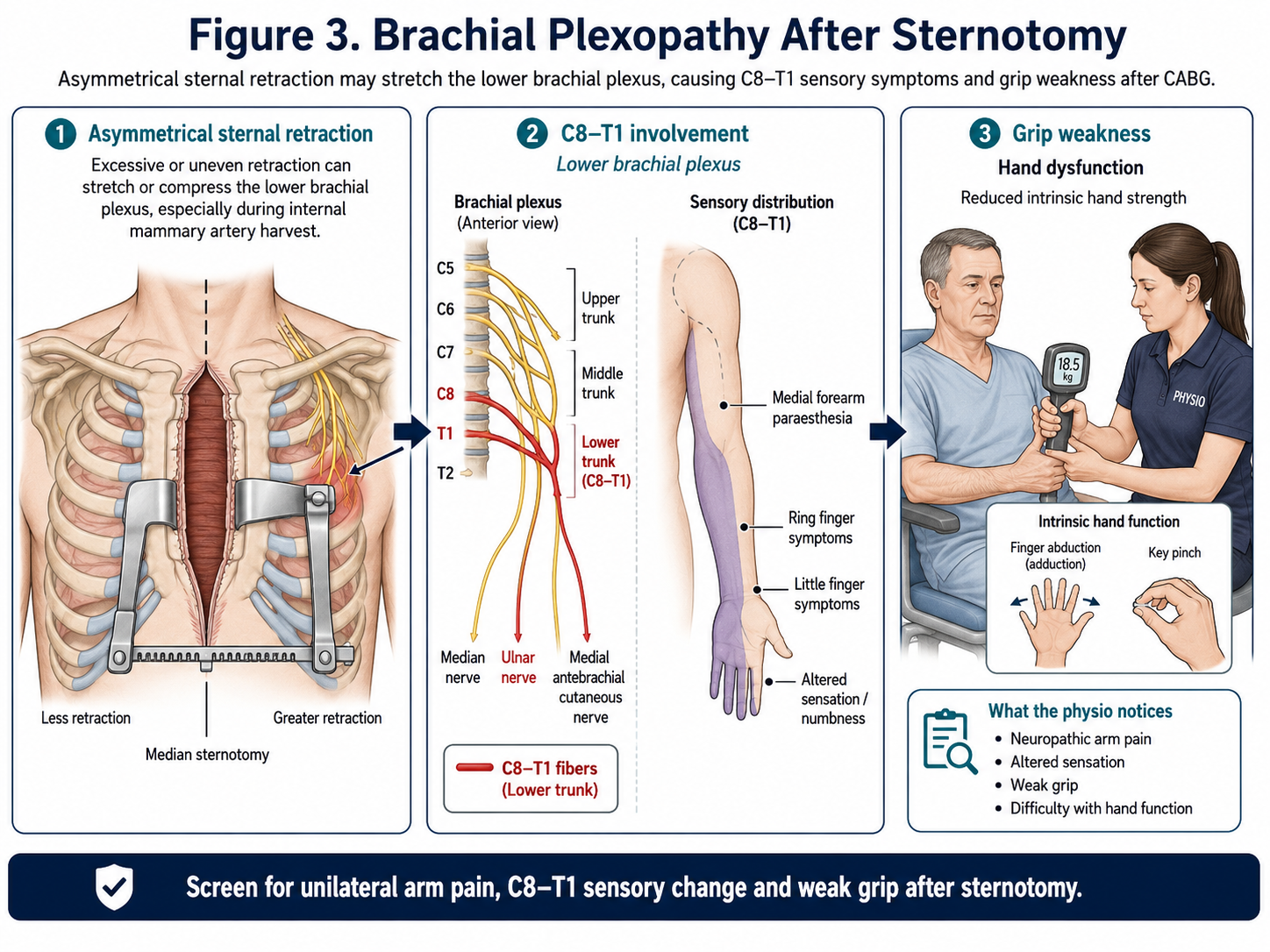
Brachial plexopathy is an injury or dysfunction of the brachial plexus—the network of nerves formed mainly by the C5–T1 spinal nerve roots that supplies motor and sensory function to the shoulder, arm, forearm and hand. After CABG, it most commonly results from traction or compression of the plexus during median sternotomy and sternal retraction. Depending on the fibres involved, the patient may develop neuropathic pain, paraesthesia, sensory loss or weakness in the affected upper limb.
Brachial plexopathy following CABG is uncommon but probably under-recognised. One series identified clinically apparent injury in 0.5% of patients, whereas older studies using active neurological surveillance reported rates from 2% to 38%. The wide range reflects differences in examination methods and whether mild, temporary sensory symptoms were included (Ünlü et al., 2007).
Patients may report burning pain, tingling or numbness extending into the medial forearm, ring finger or little finger. Weak grip, reduced finger abduction, impaired fine hand movements or difficulty using a walking aid may be observed. Physiotherapists should compare both upper limbs for dermatomal sensation, myotomal strength, grip, intrinsic hand function, active shoulder movement and scapular control.
The pattern must be differentiated from ordinary sternal or shoulder pain, cervical radiculopathy, isolated ulnar neuropathy and stroke. Facial asymmetry, speech disturbance, altered consciousness or broader unilateral weakness should be treated as possible acute cerebrovascular signs rather than brachial plexopathy.
Management initially focuses on protection and function. The limb should be supported without sustained traction, and forceful shoulder stretching or aggressive neural-tension techniques should be avoided. Gentle pain-free movement, hand exercises, maintenance of joint mobility and functional retraining may be introduced according to irritability. Persistent sensory loss, progressive weakness or severe neuropathic pain requires neurological review and may warrant nerve-conduction studies or electromyography. Recovery is often gradual, but motor deficits and axonal injuries may take several months.
A Practical Physiotherapy Screening Sequence
A reliable bedside sequence is: review the chart and telemetry, assess breathing and oxygenation, palpate the pulse, measure haemodynamics, screen limb function and then mobilise. Findings should always be compared with the previous session. A new change is usually more clinically important than an isolated abnormal value that has already been investigated.
Viva-Ready Summary
- Atelectasis is the most frequent pulmonary abnormality after cardiac surgery and commonly affects dependent basal lung regions.
- Left-lower-lobe atelectasis results from dependent positioning, pain, pleural disruption, reduced diaphragmatic excursion and, classically, cold-induced left phrenic neuropraxia.
- Physiotherapy management includes positioning, lung-expansion exercises, supported coughing when required and early mobilisation.
- Postoperative AF commonly appears on days two to four and may present as an irregular pulse, tachycardia or unexplained activity intolerance.
- New or symptomatic AF requires cessation of activity and medical assessment before mobilisation continues.
- Post-sternotomy brachial plexopathy usually affects the lower plexus and may cause medial forearm or hand paraesthesia, grip weakness and intrinsic hand dysfunction.
- Physiotherapists recognise, document and escalate these complications; definitive rhythm, ventilatory and neurological management remains multidisciplinary.
One-line recall point: After CABG, screen the lungs for collapse, the pulse for irregularity and the upper limb for neurological deficit before progressing mobilisation.
References
Benjamin, J. J., Cascade, P. N., Rubenfire, M., Wajszczuk, W., & Kerin, N. Z. (1982). Left lower lobe atelectasis and consolidation following cardiac surgery: The effect of topical cooling on the phrenic nerve. Radiology, 142(1), 11–14.
Borges, M. G. B., Borges, D. L., Ribeiro, M. O., Lima, L. S. S., Macedo, K. C. M., & Nina, V. J. S. (2022). Early mobilization prescription in patients undergoing cardiac surgery: Systematic review. Brazilian Journal of Cardiovascular Surgery, 37(2), 227–238.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Grant, M. C., Crisafi, C., Alvarez, A., Arora, R. C., Brindle, M. E., Chatterjee, S., Ender, J., Fletcher, N., Gregory, A. J., Gunaydin, S., Jahangiri, M., Ljungqvist, O., Lobdell, K. W., Morton, V., Reddy, V. S., Salenger, R., Sander, M., Zarbock, A., & Engelman, D. T. (2024). Perioperative care in cardiac surgery: A joint consensus statement by the ERAS Cardiac Society, ERAS International Society, and the Society of Thoracic Surgeons. The Annals of Thoracic Surgery, 117(4), 669–689.
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Suero, O. R., Ali, A. K., Barron, L. R., Segar, M. W., Moon, M. R., & Chatterjee, S. (2024). Postoperative atrial fibrillation after cardiac surgery: Clinical practice review. Journal of Thoracic Disease, 16(2), 1503–1520.
Tanner, T. G., & Colvin, M. O. (2020). Pulmonary complications of cardiac surgery. Lung, 198(6), 889–896.
Ünlü, Y., Velioğlu, Y., Koçak, H., Becit, N., & Ceviz, M. (2007). Brachial plexus injury following median sternotomy. Interactive CardioVascular and Thoracic Surgery, 6(2), 235–237.
Westerdahl, E., Lindmark, B., Eriksson, T., Friberg, Ö., Hedenstierna, G., & Tenling, A. (2005). Deep-breathing exercises reduce atelectasis and improve pulmonary function after coronary artery bypass surgery. Chest, 128(5), 3482–3488.



