
Off-Pump vs On-Pump CABG: What Changes for the Physiotherapist?
Understand off-pump versus on-pump CABG, including surgical differences, pulmonary complications, mobilisation timing and key implications for physiotherapy.
Coronary artery bypass grafting (CABG) may be performed with cardiopulmonary bypass—on-pump CABG—or on the beating heart without bypass—off-pump CABG. For the physiotherapist, the distinction matters because it can influence the early haemodynamic and pulmonary course. It does not, however, create two completely different rehabilitation protocols. In both procedures, mobilisation is guided by physiological stability, postoperative complications and functional response rather than by the surgical label alone.
The Surgical Difference
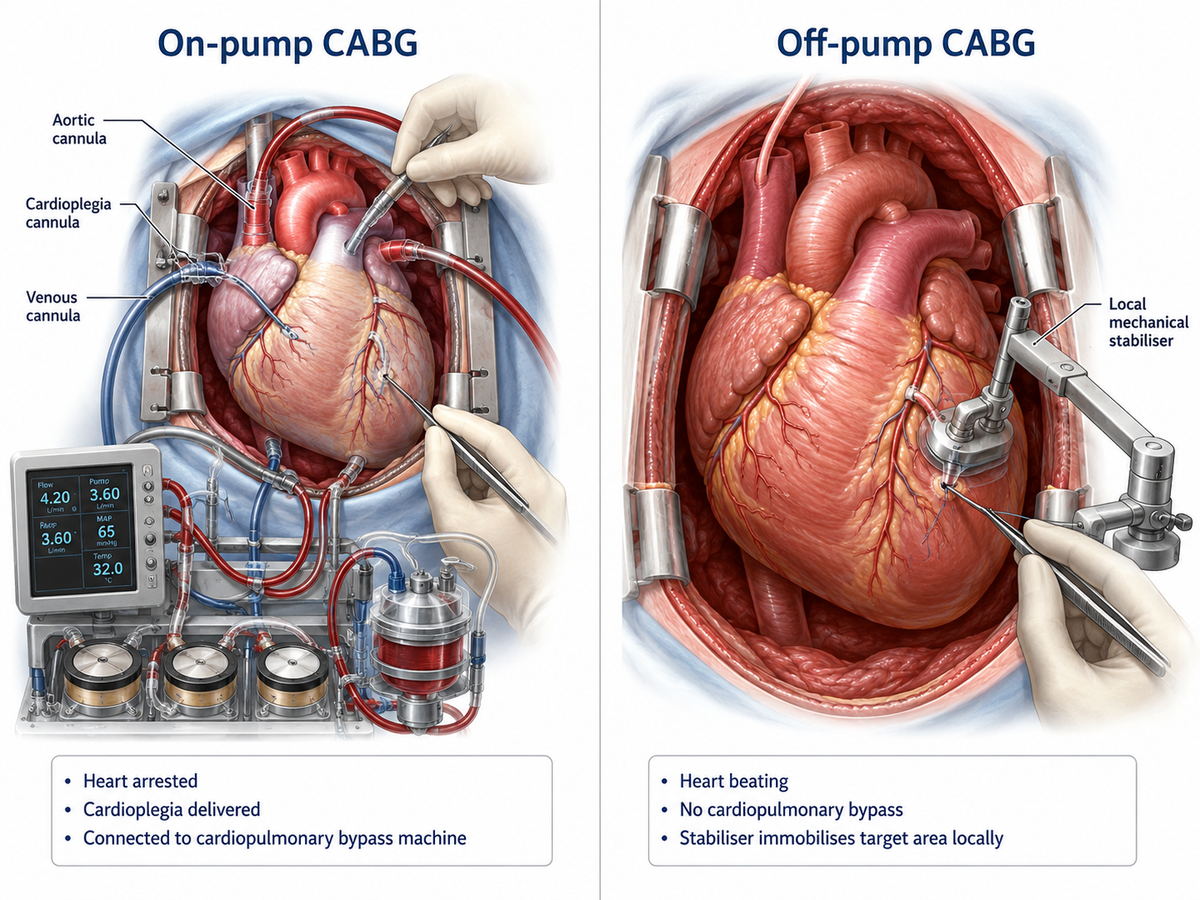
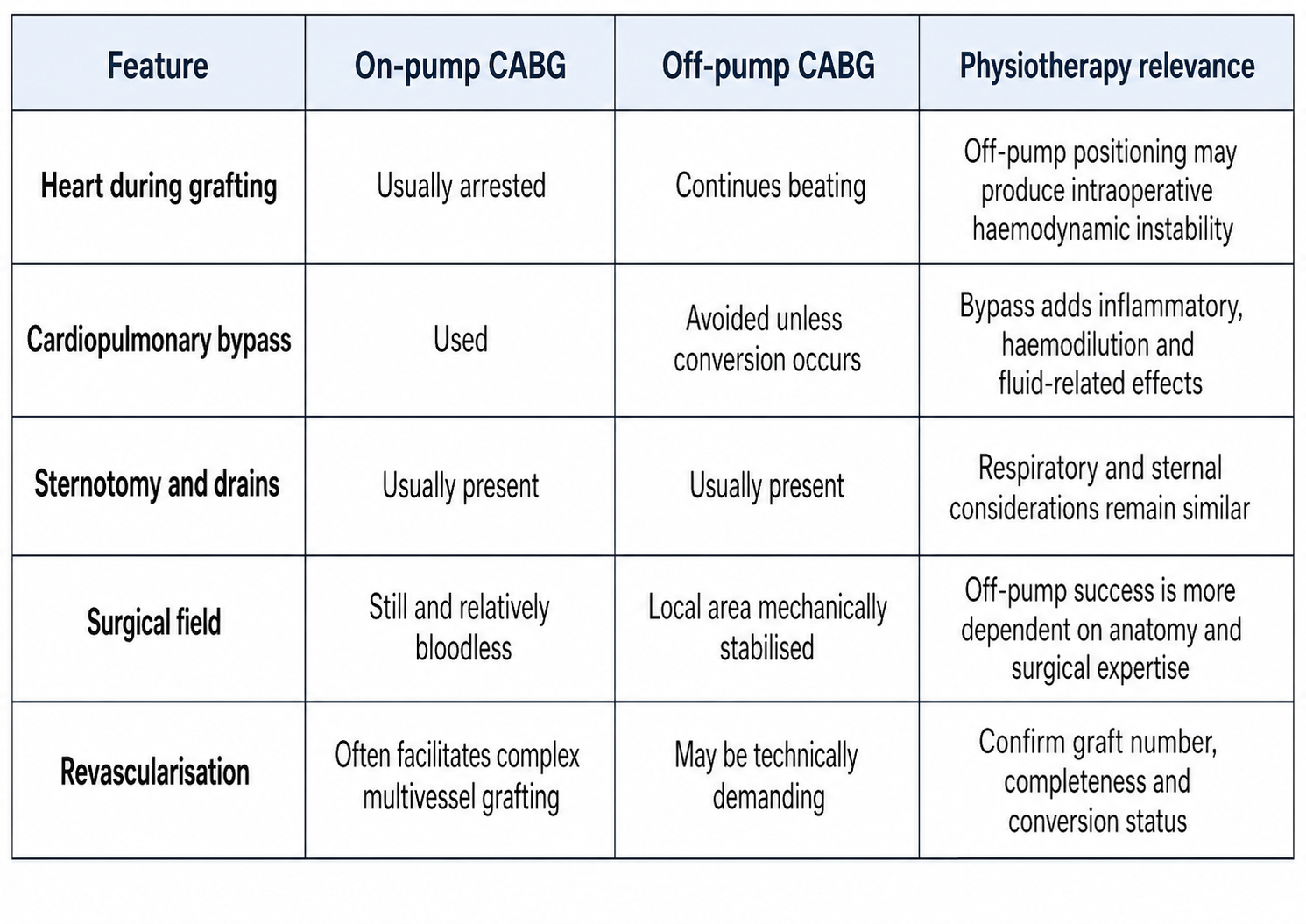
During on-pump CABG, the cardiopulmonary-bypass machine temporarily maintains circulation and oxygenation. The aorta is usually cross-clamped, cardioplegia arrests the heart, and grafts are constructed on a still, relatively bloodless field.
During off-pump CABG, the heart continues beating. A mechanical stabiliser limits movement around the target coronary artery while the surgeon performs the anastomosis. Accessing lateral or posterior vessels may require lifting or rotating the heart, which can reduce venous return, ventricular filling and cardiac output. Temporary coronary occlusion may also provoke myocardial ischaemia or arrhythmia (Frownfelter et al., 2022; Shim et al., 2023).
Off-pump surgery may be converted to on-pump CABG if severe hypotension, ventricular dysfunction, difficult anatomy or technical problems occur. Physiotherapists should therefore confirm whether conversion occurred rather than relying only on the planned surgical technique.
Off-pump also does not mean minimally invasive. Most patients still undergo median sternotomy, conduit harvesting, general anaesthesia, intubation and insertion of chest drains and pacing wires. Pain, reduced chest-wall movement, weak cough and early functional decline remain relevant after both procedures (Downie et al., 1987; Hillegass, 2022).
Pulmonary Complications: Does Off-Pump Surgery Protect the Lungs?
Pulmonary dysfunction after CABG is caused by more than cardiopulmonary bypass. General anaesthesia, sternotomy, pleural opening, internal mammary artery harvesting, pain, diaphragmatic dysfunction, fluid administration and immobility can reduce lung volumes and promote dependent atelectasis after either technique (Downie et al., 1987; Frownfelter et al., 2022).
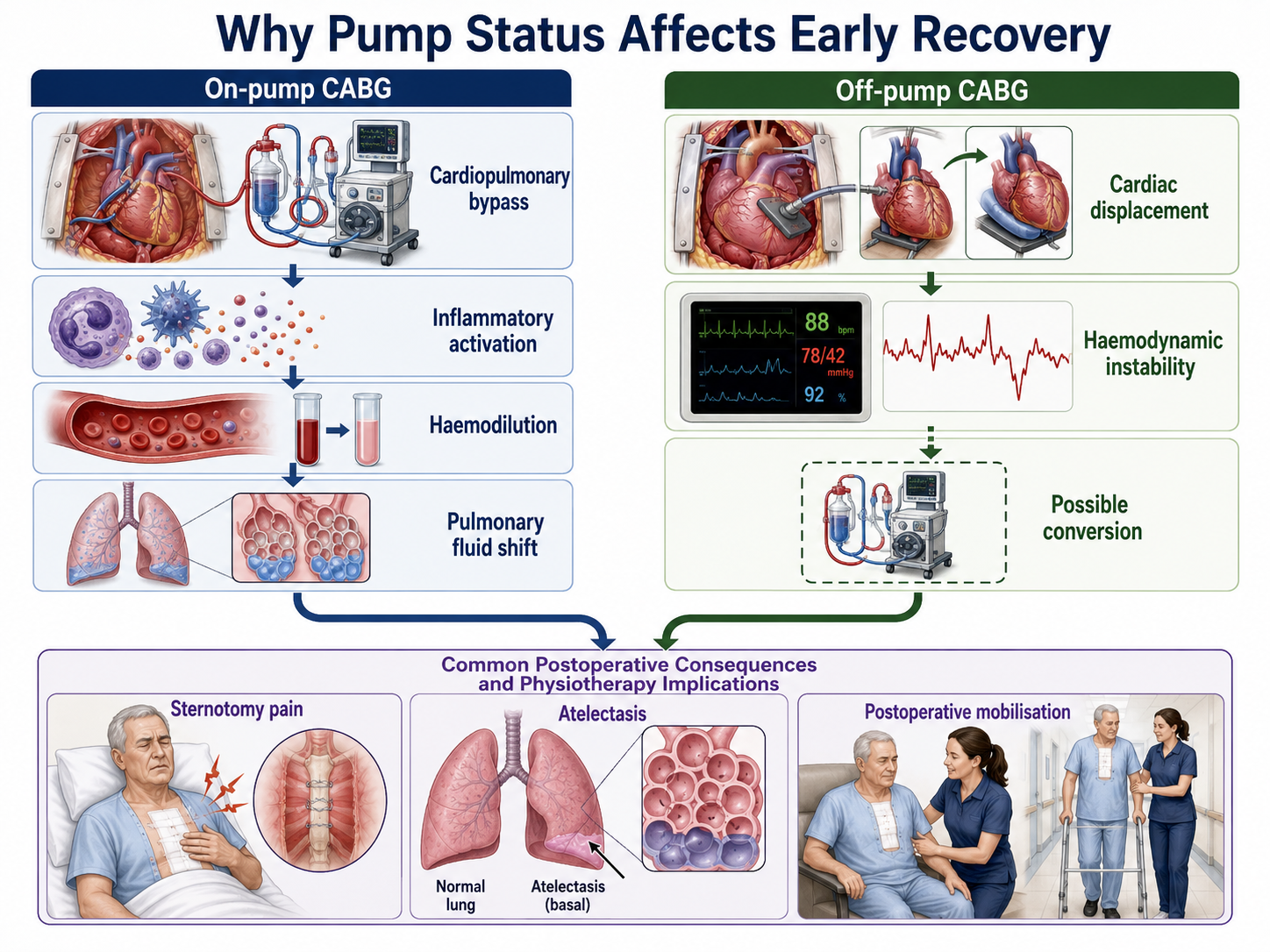
Cardiopulmonary bypass adds inflammatory activation, haemodilution, altered pulmonary perfusion and increased capillary permeability. These effects may contribute to pulmonary oedema, impaired gas exchange and delayed respiratory recovery. Avoiding bypass reduces exposure to these mechanisms but does not eliminate postoperative lung dysfunction.
Direct comparative evidence has shown marked postoperative reductions in pulmonary function after both techniques, without consistent differences in atelectasis, oxygenation or pulmonary complications (Montes et al., 2004). More recent evidence suggests a modest early advantage in selected patients. A 2025 meta-analysis in patients with COPD found that off-pump CABG shortened mechanical-ventilation time by approximately 5.3 hours but did not significantly reduce reintubation, prolonged ventilation, acute respiratory distress syndrome or mortality (Cappellaro et al., 2025).
Therefore, off-pump CABG should not be regarded as protection against atelectasis, secretion retention, hypoxaemia, ineffective cough, pleural complications or pneumonia. Both groups may require upright positioning, pain-aware deep breathing, supported coughing, selective airway clearance and early mobilisation.
What Should the Physiotherapist Check Before Treatment
The operative record and ICU handover should be reviewed before treatment. Important details include the number and type of grafts, conduit-harvest sites, bypass and cross-clamp times, conversion status, intraoperative instability, blood loss, postoperative ventricular function and rhythm.
Respiratory assessment should include oxygen or ventilatory support, respiratory rate and pattern, SpO₂ trend, air entry, cough effectiveness, retained secretions, pain and chest-drain status. Haemodynamic assessment should include heart rate, rhythm, blood pressure, mean arterial pressure, vasoactive support, signs of low cardiac output and response to positional change (Frownfelter et al., 2022; Hillegass, 2022).
Long bypass or cross-clamp times may increase concern about myocardial dysfunction, vasoplegia and delayed recovery, but they should not independently determine whether physiotherapy proceeds. Similarly, an off-pump patient may still develop anaemia, bleeding, atrial fibrillation, hypotension or ventricular dysfunction.
The key principle is that pump status contributes to risk interpretation; the patient’s present physiological condition determines treatment readiness.
Does Mobilisation Begin Earlier After Off-Pump CABG?
Some uncomplicated off-pump patients may be extubated and mobilised earlier because they avoid bypass-related effects. However, there is no rule that off-pump patients must mobilise before on-pump patients.
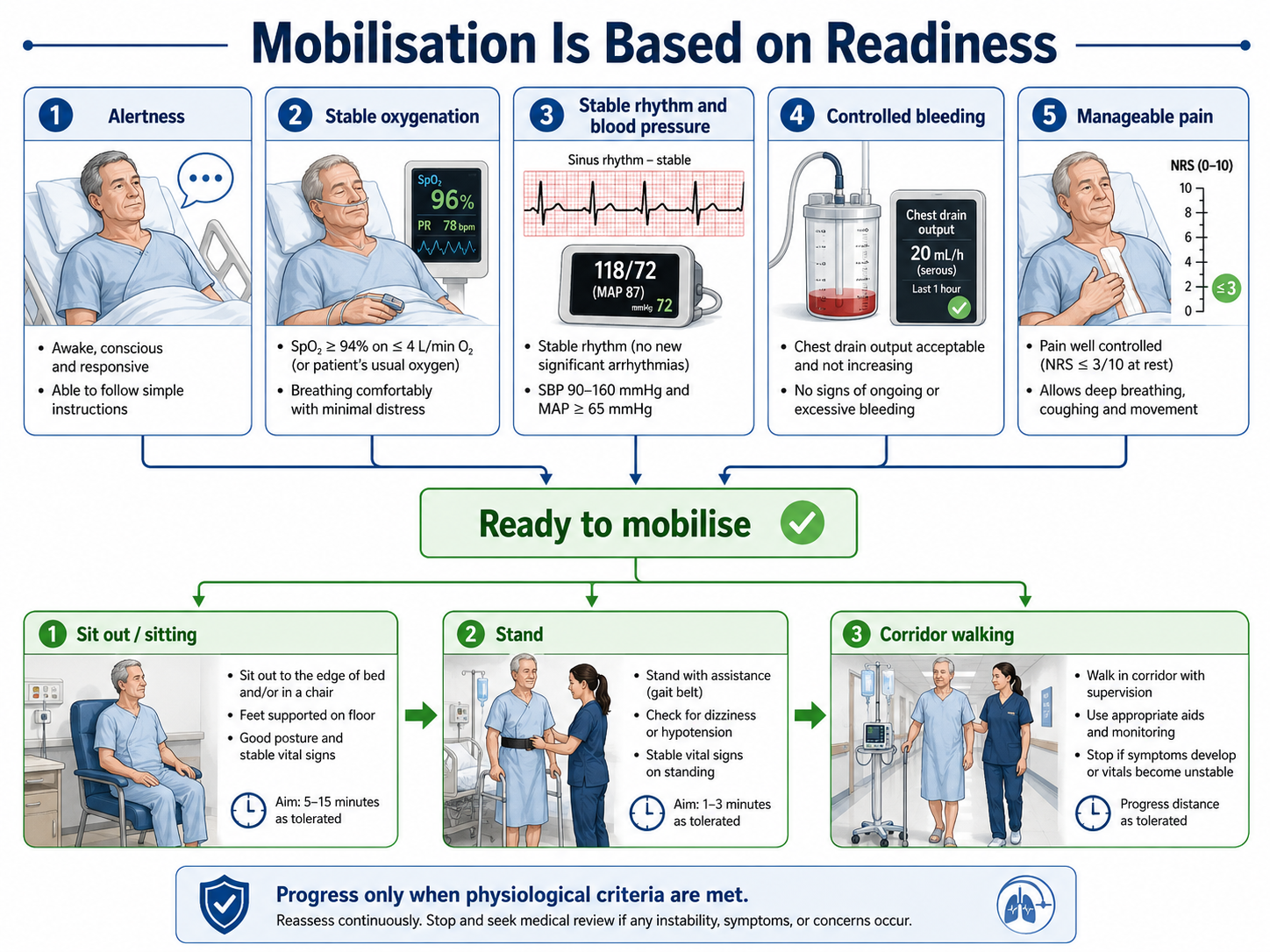
Early mobilisation after cardiac surgery commonly begins on postoperative day 1 or 2 and can improve functional walking capacity at discharge (Kanejima et al., 2020). Progression usually moves from upright positioning and active limb movements to sitting over the edge of the bed, standing, chair transfer and corridor walking.
Mobilisation is appropriate when the patient is alert, oxygenation and respiratory effort are acceptable, blood pressure and rhythm are stable, bleeding is controlled, pain is manageable and ventilatory or vasoactive support is not escalating. Treatment should be stopped or modified for new chest pain, marked dyspnoea, symptomatic hypotension, significant arrhythmia, altered consciousness, worsening desaturation, excessive drain output or increasing support requirements (Frownfelter et al., 2022; Hillegass, 2022).
An uncomplicated on-pump patient may progress as quickly as an off-pump patient, whereas an off-pump patient with low cardiac output, bleeding, arrhythmia or conversion may require delayed mobilisation.
Pump status informs risk; physiological readiness determines mobilisation.
Long-Term Outcomes: Is One Technique Better?
Long-term evidence does not show that either technique is universally superior. In the CORONARY trial, five-year rates of death, stroke, myocardial infarction, renal failure or repeat revascularisation were similar between on-pump and off-pump CABG, and quality-of-life outcomes were comparable (Lamy et al., 2016).
The ROOBY trial was less favourable to off-pump surgery. Ten-year mortality did not differ significantly, but the off-pump group reached the composite outcome of death or repeat revascularisation earlier (Quin et al., 2022).
A 2024 meta-analysis found that off-pump CABG reduced short-term stroke but increased mid-term repeat revascularisation and was associated with a small increase in long-term mortality (He et al., 2024). These differences may reflect surgeon experience, coronary anatomy, conversion rates, graft patency and completeness of revascularisation.
Current guidelines therefore support selective rather than routine use of off-pump CABG. It may be reasonable in patients with significant pulmonary disease when performed by experienced surgeons, while techniques that avoid aortic manipulation may benefit patients with a heavily calcified ascending aorta (Lawton et al., 2022).
For physiotherapists, these comparisons do not alter the need for comprehensive cardiac rehabilitation. Both groups require graded exercise, functional restoration, risk-factor management, psychosocial support and long-term physical activity.
Practical Physiotherapy Implications
After on-pump CABG, be particularly alert to delayed extubation, pulmonary fluid accumulation, vasoplegia, neurological change, rhythm disturbance and delayed recovery after prolonged bypass.
After off-pump CABG, consider intraoperative instability caused by cardiac displacement, myocardial dysfunction, bleeding, arrhythmia and possible conversion to bypass.
Early physiotherapy goals remain similar: optimise ventilation, support an effective cough, identify atelectasis or retained secretions, prevent immobility-related complications and restore transfers, walking and activities of daily living.
Patients should not be told that off-pump CABG is a minor operation. Although it avoids cardiopulmonary bypass, it usually retains the sternotomy, graft-harvest wounds, postoperative pain and rehabilitation requirements of conventional CABG.
The most useful clinical question is:
“What physiological consequences did this patient experience, and are they ready to progress today?”
Viva-Ready Summary
On-pump CABG uses cardiopulmonary bypass and usually cardioplegic arrest. Off-pump CABG is performed on a beating, mechanically stabilised heart and may cause haemodynamic instability when the heart is displaced.
Off-pump CABG may shorten ventilation time in selected patients, but pulmonary dysfunction occurs after both techniques. Mobilisation may begin earlier after an uncomplicated off-pump procedure, although progression must always be based on respiratory, haemodynamic and neurological stability.
Long-term outcomes are mixed: some trials show similar outcomes, while others report greater repeat revascularisation after off-pump CABG. Surgeon experience and completeness of revascularisation remain important.
One-line recall point: Off-pump CABG avoids cardiopulmonary bypass, but it does not avoid pulmonary complications, sternotomy rehabilitation or stability-based mobilisation.
References
Cappellaro, A. P., Costa de Almeida, L. F., Pinto, M. L., Martins, M. A. B., Graziani e Sousa, A., Gadelha, J. G., Vieira, A. C. P., Rocha, L. F. R., & Thet, M. S. (2025). Off-pump versus on-pump coronary artery bypass grafting in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. General Thoracic and Cardiovascular Surgery, 73, 201–208. https://doi.org/10.1007/s11748-025-02116-3
Downie, P. A., Innocenti, D. M., & Jackson, S. E. (Eds.). (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Faber and Faber.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
He, L., Tiemuerniyazi, X., Chen, L., Yang, Z., Huang, S., Nan, Y., Song, Y., & Feng, W. (2024). Clinical outcomes of on-pump versus off-pump coronary-artery bypass surgery: A meta-analysis. International Journal of Surgery, 110(8), 5063–5070. https://doi.org/10.1097/JS9.0000000000001481
Hillegass, E. A. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Kanejima, Y., Shimogai, T., Kitamura, M., Ishihara, K., & Izawa, K. P. (2020). Effect of early mobilization on physical function in patients after cardiac surgery: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 17(19), 7091. https://doi.org/10.3390/ijerph17197091
Lamy, A., Devereaux, P. J., Prabhakaran, D., Taggart, D. P., Hu, S., Straka, Z., Piegas, L. S., Avezum, A., Akar, A. R., Lanas Zanetti, F., Jain, A. R., Noiseux, N., Padmanabhan, C., Bahamondes, J.-C., Novick, R. J., Tao, L., Olavegogeascoechea, P. A., Airan, B., Sulling, T.-A., . . . Yusuf, S. (2016). Five-year outcomes after off-pump or on-pump coronary-artery bypass grafting. The New England Journal of Medicine, 375(24), 2359–2368. https://doi.org/10.1056/NEJMoa1601564
Lawton, J. S., Tamis-Holland, J. E., Bangalore, S., Bates, E. R., Beckie, T. M., Bischoff, J. M., Bittl, J. A., Cohen, M. G., DiMaio, J. M., Don, C. W., Fremes, S. E., Gaudino, M. F., Goldberger, Z. D., Grant, M. C., Jaswal, J. B., Kurlansky, P. A., Mehran, R., Metkus, T. S., Nnacheta, L. C., . . . Zwischenberger, B. A. (2022). 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 145(3), e18–e114. https://doi.org/10.1161/CIR.0000000000001038
Montes, F. R., Maldonado, J. D., Paez, S., & Ariza, F. (2004). Off-pump versus on-pump coronary artery bypass surgery and postoperative pulmonary dysfunction. Journal of Cardiothoracic and Vascular Anesthesia, 18(6), 698–703. https://doi.org/10.1053/j.jvca.2004.08.004
Quin, J. A., Wagner, T. H., Hattler, B., Carr, B. M., Collins, J. F., Almassi, G. H., Grover, F. L., & Shroyer, A. L. (2022). Ten-year outcomes of off-pump vs on-pump coronary artery bypass grafting in the Department of Veterans Affairs: A randomized clinical trial. JAMA Surgery, 157(4), 303–310. https://doi.org/10.1001/jamasurg.2021.7578
Shim, J. K., Kim, K.-S., Couture, P., Denault, A., Kwak, Y. L., Yoo, K.-J., & Youn, Y.-N. (2023). Hemodynamic management during off-pump coronary artery bypass surgery: A narrative review of proper targets for safe execution and troubleshooting. Korean Journal of Anesthesiology, 76(4), 267–279. https://doi.org/10.4097/kja.23103



