
Inspiratory Muscle Training: Does It Really Work?
Learn how inspiratory muscle training works, how to prescribe 30–50% MIP, which devices are used and what evidence supports IMT in COPD, CABG and ICU patients.
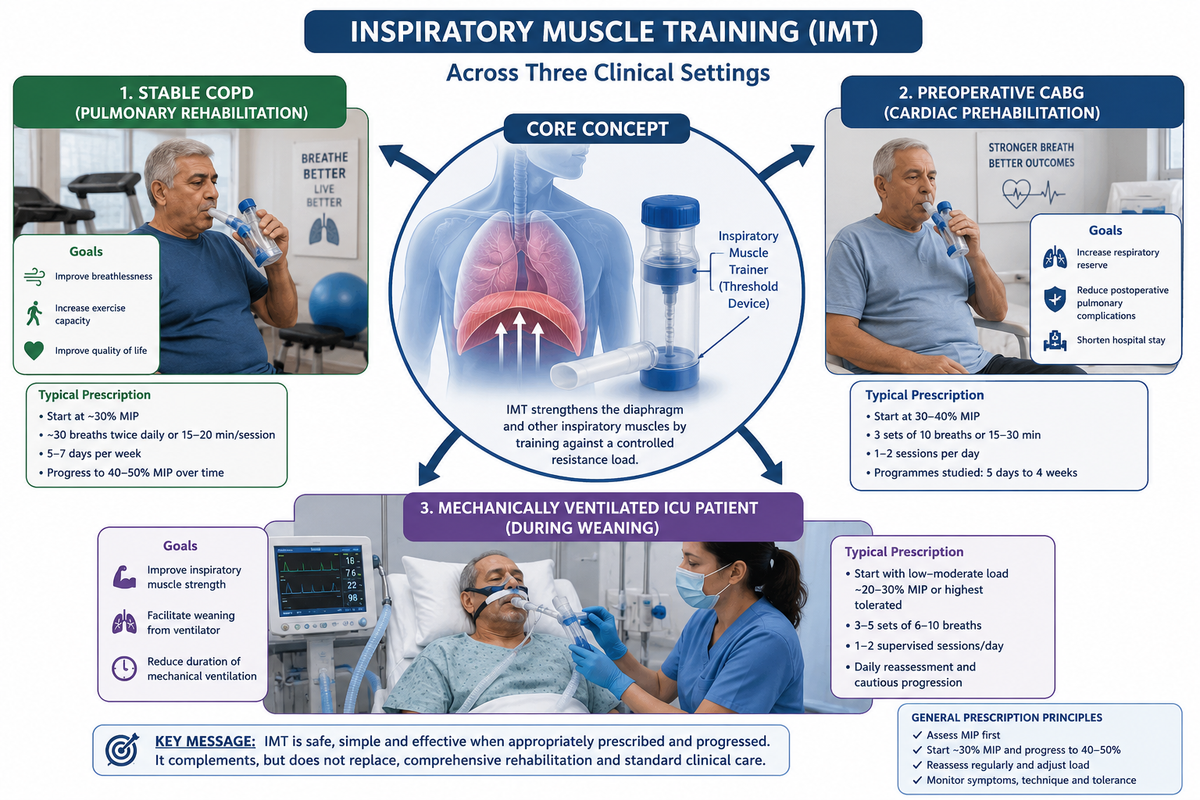
Inspiratory muscle training, or IMT, is targeted resistance training for the muscles responsible for inspiration—principally the diaphragm, supported by the external intercostals and accessory inspiratory muscles. Unlike relaxed diaphragmatic breathing or incentive spirometry, IMT applies a measurable external load that the patient must overcome during inspiration.
The principle is simple: the diaphragm is skeletal muscle and responds to appropriately prescribed overload. The clinical answer, however, is more nuanced. IMT reliably improves the function it directly trains—inspiratory muscle strength—but improvement in walking capacity, postoperative complications or ventilator weaning depends on the population, baseline weakness, training dose and accompanying rehabilitation programme.
How IMT Overloads the Diaphragm
During IMT, the patient inspires against a pressure- or flow-dependent resistance. Repeated loading recruits inspiratory motor units and promotes strength and endurance adaptations, similar to resistance training of limb muscles. As maximal inspiratory pressure increases, the pressure required for ordinary breathing represents a smaller proportion of the patient’s maximum capacity. Breathing may therefore feel less demanding during exercise or illness (Frownfelter et al., 2022; Hillegass, 2022).

This mechanism is particularly relevant in three clinical situations.
In COPD, hyperinflation shortens and flattens the diaphragm, placing it at a mechanical disadvantage. Increased airway resistance and dynamic hyperinflation also raise the work of breathing. In patients undergoing CABG, anaesthesia, cardiopulmonary bypass, pain, sternotomy and reduced postoperative lung volumes may temporarily impair inspiratory muscle performance. In mechanically ventilated ICU patients, diaphragm unloading, systemic inflammation and critical illness contribute to rapidly developing weakness and ventilator-induced diaphragmatic dysfunction.
IMT attempts to increase the patient’s inspiratory reserve before or during these periods of increased demand. It does not directly reverse airway obstruction, remove secretions or treat the underlying disease.
Assessment and Practical Prescription
Training should begin with measurement of maximal inspiratory pressure, or MIP, generally from residual volume using a pressure manometre. The patient exhales fully and then inspires as forcefully as possible against an occluded airway. At least three acceptable efforts should be obtained, with adequate rest and reasonable reproducibility between attempts.
A commonly used starting intensity is 30% of the measured MIP. The resistance can be increased towards 40–50% MIP as the patient completes the prescribed breaths without loss of technique, excessive accessory-muscle activity or marked distress. MIP should be reassessed regularly because an unchanged device setting becomes a progressively smaller training stimulus as strength improves.

The numbers are a framework rather than a rigid protocol. In severe weakness, a patient may initially require a lower resistance simply to open the valve. Conversely, stronger and clinically stable patients may tolerate higher-intensity or interval-based training.

Quality matters more than hurried repetitions. The patient should maintain an upright or appropriately supported position, seal the lips around the mouthpiece, inspire forcefully through the device and recover between sets. Training should be stopped or modified if there is significant desaturation, haemodynamic instability, new arrhythmia, severe distress, dizziness, paradoxical breathing or progressive loss of inspiratory effort.
Threshold and Tapered Flow-Resistive Devices
A threshold-loading device contains a spring-loaded or weighted valve. The patient must generate a predetermined negative pressure before the valve opens. Once that threshold is reached, airflow can occur. Because the opening pressure is relatively independent of inspiratory flow, the clinician can prescribe the load as a reproducible percentage of MIP. Threshold devices are widely used in pulmonary rehabilitation, cardiac prehabilitation and ICU research.
A tapered flow-resistive loading device provides a resistance profile that changes during the breath. The initial load is relatively high and then reduces as inspiration continues, corresponding more closely to the pressure-generating capacity of the inspiratory muscles across lung volume. Electronic versions may record pressure, volume, power and adherence and provide visual feedback. Tapered loading can permit higher training intensities and has produced favourable physiological responses in COPD, although cost and availability may limit routine use (Langer et al., 2015).

Simple flow-resistive devices create resistance through a narrowed aperture. Their load varies with inspiratory flow, so a faster inspiration may produce a greater resistance. They are less precise unless breathing pattern and flow are carefully controlled.
Exam tip: An incentive spirometer encourages sustained maximal inspiration and lung expansion. It is not automatically an inspiratory muscle trainer because it may not provide a controlled resistance of at least approximately 30% MIP.
Evidence in COPD: Useful, but Not a Replacement for Rehabilitation
The evidence in COPD depends heavily on the comparison group. The Cochrane review by Ammous et al. (2023) found that stand-alone IMT, compared with sham or no training, probably improves functional exercise capacity and may improve dyspnoea and health-related quality of life. Improvements were also reported in MIP. A more recent meta-analysis similarly found benefits in inspiratory strength, breathlessness and quality of life, although protocols and study quality remained variable (Han et al., 2024).
The interpretation changes when IMT is added to a well-designed pulmonary rehabilitation programme. Pulmonary rehabilitation already includes aerobic and resistance exercise, education and symptom-management strategies. The Cochrane review found little clinically important additional improvement in dyspnoea, six-minute walk distance or quality of life when IMT was added routinely to pulmonary rehabilitation.
Therefore, IMT should not replace whole-body exercise training. Its most logical role is as an individualised adjunct for patients with documented inspiratory muscle weakness, disproportionate breathlessness, difficulty tolerating conventional exercise or limited access to a full rehabilitation programme.
Evidence verdict for COPD: Moderate support for stand-alone IMT and clear improvement in MIP, but uncertain additional patient-important benefit when high-quality pulmonary rehabilitation is already being delivered.
Evidence Before and After CABG
The strongest perioperative evidence supports preoperative, rather than exclusively postoperative, IMT. Training before surgery increases inspiratory reserve before the predictable postoperative fall in lung volume, cough effectiveness and respiratory muscle performance.
A 2024 systematic review of eight randomised trials involving 696 cardiac-surgery patients found that preoperative respiratory muscle training reduced the risk of postoperative pulmonary complications and pneumonia by approximately half and shortened hospital stays by about 1.7 days. Most programmes began at around 30% MIP and lasted between 2 and 4 weeks, although shorter protocols were also studied (Cursino de Moura et al., 2024).
A CABG-specific meta-analysis also found lower risks of pneumonia and atelectasis, improved postoperative inspiratory strength and shorter hospitalisation, although the quality of evidence varied between outcomes (Xiang et al., 2023).
Postoperative IMT may help restore MIP, but pain, fatigue, drains, haemodynamic status and the patient’s ability to follow commands influence feasibility. It must complement—not replace—upright positioning, early mobilisation, supported coughing, lung-expansion strategies and routine Phase I cardiac rehabilitation.
Evidence verdict for CABG: Yes, particularly as prehabilitation in patients awaiting elective surgery. Prevention of pulmonary complications is more clinically important than merely increasing MIP.
Evidence in Mechanically Ventilated ICU Patients
IMT in the ICU is usually considered after the patient can initiate breaths, participate with instructions and tolerate brief reductions in ventilatory assistance. Training may be delivered through a threshold device connected to an artificial airway or through an electronic resistive-loading system.
Recent evidence suggests that IMT can increase MIP in ventilated patients. Some analyses also report shorter weaning duration and fewer reintubations, particularly in patients ventilated for seven days or longer. However, certainty remains low because trials use different devices, intensities, definitions of weakness and weaning protocols (Farley et al., 2026).
A recent review of prolonged mechanical ventilation reported favourable effects of higher-intensity IMT on MIP and extubation outcomes, but substantial heterogeneity limits generalisation (Andrade-Rebolledo et al., 2026). A multicentre trial comparing low-, high- and mixed-intensity programmes also demonstrated that no single dosing strategy has yet emerged as universally superior (Réginault et al., 2024).
IMT should therefore be regarded as one component of a complete weaning and rehabilitation bundle that includes optimisation of sedation, spontaneous breathing trials, secretion management, nutrition, mobilisation and treatment of the underlying illness.
Evidence verdict for ICU: Promising for improving inspiratory strength and potentially useful in selected difficult-to-wean patients, but not yet a guaranteed or independently sufficient weaning intervention.
Does IMT Actually Work?
Yes—but it works most consistently for inspiratory muscle strength, and its broader clinical effect depends on the population.
- In COPD, it improves MIP and can improve breathlessness and exercise capacity when used alone, especially in inspiratory muscle weakness. It adds less when comprehensive pulmonary rehabilitation is already effective.
- Before CABG, preoperative IMT reduces pneumonia and other pulmonary complications and may shorten hospital stay.
- In the ICU, it increases inspiratory strength and may assist difficult or prolonged weaning, but evidence for weaning success remains heterogeneous.
Viva-ready summary
IMT is progressive resistance exercise for the diaphragm and other inspiratory muscles. Assess MIP first, usually begin at approximately 30% MIP, progress towards 40–50%, and prescribe repeated supervised or home-based sessions. Threshold devices provide a relatively flow-independent load, while tapered flow-resistive devices alter resistance across inspiration. The best evidence supports strength and symptom gains in selected COPD patients, preoperative complication prevention before CABG and cautious use in difficult-to-wean ICU patients.
One-line recall point: IMT strengthens the inspiratory pump, but the clinically important outcome depends on who is trained, when training begins and whether the load is progressively increased.
References
Ammous, O., Feki, W., Lotfi, T., Khamis, A. M., Gosselink, R., Rebai, A., & Kammoun, S. (2023). Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD). Cochrane Database of Systematic Reviews, 2023(1), CD013778. https://doi.org/10.1002/14651858.CD013778.pub2
Andrade-Rebolledo, F. A., Villagra-Morales, G., & Pérez, L. A. (2026). Inspiratory muscle training in weaning from prolonged mechanical ventilation: A systematic review and meta-analysis. Frontiers in Medicine, 12, 1719837. https://doi.org/10.3389/fmed.2025.1719837
Cursino de Moura, J. F., Oliveira, C. B., Coelho Figueira Freire, A. P., Elkins, M. R., & Pacagnelli, F. L. (2024). Preoperative respiratory muscle training reduces the risk of pulmonary complications and the length of hospital stay after cardiac surgery: A systematic review. Journal of Physiotherapy, 70(1), 16–24.
Downie, P. A. (Ed.). (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Faber and Faber.
Farley, C., Oliveira, A., Brooks, D., & Newman, A. N. L. (2026). The effects of inspiratory muscle training in critically ill adults: A systematic review and meta-analysis. Journal of Intensive Care Medicine, 41(4). https://doi.org/10.1177/08850666251317473
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
Han, B., Chen, Z., Ruan, B., Chen, Y., & Lv, Y. (2024). Effects of inspiratory muscle training in people with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Life, 14(11), 1470. https://doi.org/10.3390/life14111470
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Langer, D., Charususin, N., Jácome, C., Hoffman, M., McConnell, A., Decramer, M., & Gosselink, R. (2015). Efficacy of a novel method for inspiratory muscle training in people with chronic obstructive pulmonary disease. Physical Therapy, 95(9), 1264–1273. https://doi.org/10.2522/ptj.20140245
Réginault, T., Martinez Alejos, R., Coueron, R., Burle, J.-F., Boyer, A., Frison, E., & Vargas, F. (2024). Impacts of three inspiratory muscle training programmes on inspiratory muscle strength and endurance among intubated and mechanically ventilated patients with difficult weaning: A multicentre randomised controlled trial. Journal of Intensive Care, 12, 28. https://doi.org/10.1186/s40560-024-00741-3
Xiang, Y., Zhao, Q., Luo, T., & Zeng, L. (2023). Inspiratory muscle training to reduce risk of pulmonary complications after coronary artery bypass grafting: A systematic review and meta-analysis. Frontiers in Cardiovascular Medicine, 10, 1223619. https://doi.org/10.3389/fcvm.2023.1223619



