
Emphysema Explained: From Alveolar Destruction to Physiotherapy Management
Understand centriacinar and panacinar emphysema, hyperinflation, flattened diaphragm, barrel chest, pursed-lip breathing and evidence-based physiotherapy management.
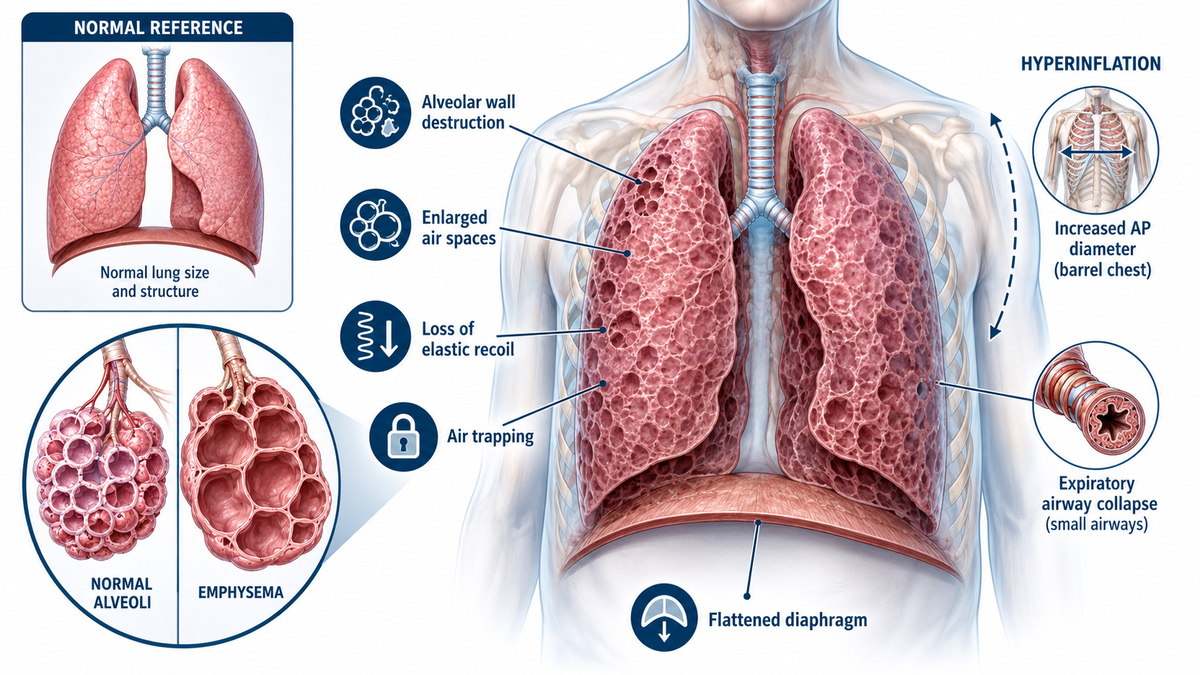
Emphysema is a structural lung disorder characterised by permanent enlargement of air spaces distal to the terminal bronchioles, accompanied by destruction of alveolar walls. It commonly occurs within chronic obstructive pulmonary disease (COPD), but it is not synonymous with COPD. COPD is diagnosed physiologically by persistent airflow obstruction, whereas emphysema describes pathological or radiological destruction of lung parenchyma.
For physiotherapists, the central sequence is straightforward: alveolar destruction reduces elastic recoil, small airways collapse during expiration, air becomes trapped, and progressive hyperinflation places the respiratory muscles at a mechanical disadvantage (Bentaher et al., 2025; Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026).
Pathophysiology: Why Air Enters but Does Not Leave Efficiently
Cigarette smoke and other inhaled irritants produce chronic inflammation, oxidative stress and an imbalance between proteases and antiproteases. Proteolytic injury damages elastin and the alveolar septa, while loss of alveolar attachments removes the radial traction that normally holds small airways open. During expiration, particularly when intrathoracic pressure rises, unsupported bronchioles narrow or collapse prematurely.
The consequences are interconnected. Loss of elastic recoil slows expiratory flow, incomplete expiration increases residual volume, and destruction of alveolar-capillary units reduces the surface available for gas exchange. Ventilation–perfusion inequality gradually develops, and diffusing capacity for carbon monoxide is commonly reduced in emphysema-predominant COPD.
Symptoms may initially be mild because the lungs have a considerable physiological reserve. However, exertional dyspnoea becomes more prominent as air trapping, hyperinflation and gas-exchange impairment progress (Frownfelter et al., 2022; Hillegass, 2022).
Centriacinar vs Panacinar Emphysema

Centriacinar, also called centrilobular, emphysema is the commoner smoking-related pattern. Panacinar, or panlobular, emphysema should prompt consideration of alpha-1 antitrypsin deficiency, particularly when the disease appears at a younger age or is disproportionate to the patient’s smoking history.
These patterns may overlap in advanced disease. The distinction is therefore most useful for understanding aetiology and radiological distribution rather than determining physiotherapy treatment in isolation (Bentaher et al., 2025).
Hyperinflation and the Flattened Diaphragm
Hyperinflation may be static or dynamic. Static hyperinflation is the chronic elevation of end-expiratory lung volume caused by reduced elastic recoil and air trapping. Dynamic hyperinflation occurs when breathing becomes faster during exercise or respiratory distress and the next inspiration begins before expiration is complete. End-expiratory lung volume rises breath by breath, while inspiratory capacity falls.
The diaphragm normally contracts from a domed position. Hyperinflation flattens and shortens it, reduces its zone of apposition with the lower rib cage and places its muscle fibres on a less favourable length–tension relationship. The patient must then generate greater neural drive for a relatively small tidal-volume response.

Accessory respiratory muscles become more active, while inspiration begins against intrinsic positive end-expiratory pressure, creating an additional threshold load. As the operating lung volume approaches total lung capacity, further tidal expansion becomes increasingly difficult, and dyspnoea rises sharply (D’Cruz et al., 2026).
This explains why a patient may tolerate quiet sitting but become markedly breathless during walking, stair climbing or repeated upper-limb activities. Dynamic hyperinflation is therefore an important mechanism behind exercise intolerance rather than simply an abnormal lung-volume measurement.
Clinical Findings and the Barrel-Chest Question
Progressive exertional dyspnoea is usually the dominant complaint. Cough and sputum may occur, especially when chronic bronchitis coexists, but they are not necessarily prominent in relatively pure emphysema.
Clinical examination may reveal the following:
- Tachypnoea with prolonged expiration
- Reduced chest expansion
- Hyperresonance on percussion
- Quiet or diminished breath sounds
- Accessory-muscle recruitment
- Reduced diaphragmatic movement
- Supported forward-leaning or tripod posture
- Spontaneous pursed-lip breathing
- Weight loss and peripheral muscle wasting in advanced disease
A barrel chest refers to an increased anteroposterior diameter, producing a rounded, persistently expanded thorax with more horizontal ribs and widened intercostal spaces. The classic examination comparison is an AP-to-transverse diameter approaching 1:1 rather than the usual adult proportion of approximately 1:2. It develops because chronic hyperinflation holds the rib cage closer to the inspiratory position.
However, a barrel chest is usually a late and relatively insensitive sign. Its absence does not exclude emphysema, and its presence does not independently establish the diagnosis.
Chest radiography may demonstrate hyperlucent lung fields, flattened diaphragms, widened intercostal spaces, increased retrosternal airspace and a long, narrow cardiac silhouette. Spirometry typically shows a reduced post-bronchodilator FEV₁/FVC ratio, while lung-volume testing may show increased residual volume, functional residual capacity and total lung capacity (Sarkar et al., 2019).
Exam caution: Digital clubbing is not a typical feature of uncomplicated emphysema. Its presence should raise suspicion of an alternative or additional condition, such as bronchiectasis, lung malignancy or interstitial lung disease.
Physiotherapy Assessment and Treatment Priorities
Physiotherapy cannot regenerate destroyed alveolar walls. Its role is to minimise the functional consequences of breathlessness, inefficient breathing, peripheral muscle weakness and physical deconditioning.
Assessment should connect physiological impairment with activity limitation and participation restriction. Useful measures include:
- Respiratory rate, oxygen saturation and breathing pattern
- Chest-wall and diaphragmatic movement
- Modified Medical Research Council dyspnoea grade
- COPD Assessment Test score
- Six-minute walk test or incremental shuttle walk test
- Peripheral and inspiratory muscle strength
- Balance, nutritional status and body composition
- Inhaler technique and treatment adherence
- Functional ability during daily activities
The physiotherapist should also observe whether breathlessness is triggered by rapid walking, repeated upper-limb activity, bending forward, talking while walking or breath-holding during effort.
Pulmonary rehabilitation is the central evidence-based intervention for symptomatic COPD. It combines individually prescribed aerobic and resistance training with education, self-management and behavioural support. The American Thoracic Society strongly recommends pulmonary rehabilitation for stable COPD and following hospitalisation for a COPD exacerbation (Rochester et al., 2023).
Interval training may be useful when continuous exercise causes intolerable dyspnoea. Resistance training addresses peripheral muscle weakness without requiring the same sustained ventilation as endurance exercise. Inspiratory muscle training may be considered when objective inspiratory muscle weakness is present.
Airway-clearance techniques should not be prescribed simply because emphysema has been diagnosed. They are indicated when sputum retention, ineffective coughing or coexisting bronchiectasis creates a genuine secretion-clearance problem.

Pursed-Lip Breathing, Breathing Retraining and Energy Conservation
Pursed-lip breathing consists of a relaxed inspiration followed by slow expiration through gently narrowed lips. The mild expiratory back-pressure helps splint collapsable airways, while the longer expiratory phase reduces respiratory rate and provides additional time for lung emptying.
It may therefore reduce dynamic hyperinflation and improve control of exertional dyspnoea in selected patients, although individual responses vary (Pereira de Araujo et al., 2015).
A practical teaching sequence is the following:
- Relax the neck and shoulders.
- Inhale gently through the nose without taking an unnecessarily large breath.
- Exhale through loosely pursed lips for approximately twice as long as inspiration.
- Avoid forceful blowing, which may increase airway compression.
- Practise at rest before combining the technique with walking or functional activity.
- Exhale during effort, such as while standing up, climbing a step or lifting an object.
Breathing retraining should emphasise a slower respiratory rate, relaxed upper-chest movement, prolonged expiration, avoidance of breath-holding and recovery positions such as supported forward leaning.
Diaphragmatic breathing should not be imposed automatically. In severe hyperinflation, the flattened diaphragm may not respond efficiently to forced abdominal breathing. Recent systematic-review evidence for diaphragmatic breathing in COPD also remains inconsistent (Kwon et al., 2026). It should be used selectively when it improves thoracoabdominal synchrony and comfort without increasing respiratory effort or distress.
Energy conservation translates breathing control into daily function. The patient should be taught to:
- Plan and prioritise essential activities
- Pace rather than rush tasks
- Alternate heavier and lighter activities
- Sit during grooming, bathing or meal preparation
- Keep frequently used objects within easy reach
- Divide stair climbing into manageable stages
- Exhale during effort and avoid breath-holding
- Take short rests before severe breathlessness develops
Repeated bending, rushed speech during activity and large meals may worsen dyspnoea in some patients and should be modified when relevant.
Viva-Ready Summary
- Emphysema is permanent enlargement of distal air spaces accompanied by alveolar-wall destruction.
- Centriacinar emphysema is classically upper-lobe predominant and smoking-related.
- Panacinar emphysema affects the entire acinus, is more basal and is associated with alpha-1 antitrypsin deficiency.
- Loss of elastic recoil and alveolar attachments causes expiratory airway collapse, air trapping and hyperinflation.
- Hyperinflation flattens the diaphragm, reduces inspiratory capacity and increases the work of breathing.
- Barrel chest results from chronic hyperinflation but is neither an early nor a diagnostic sign.
- Pursed-lip breathing prolongs expiration and may reduce dynamic hyperinflation.
- Pulmonary rehabilitation remains the foundation of physiotherapy management.
- Airway-clearance techniques are required only when secretions are present.
One-line recall point: Emphysema destroys elastic alveolar support, making expiration the main problem—air trapping flattens the diaphragm, while physiotherapy restores breathing efficiency and function rather than damaged lung tissue.
References
Bentaher, A., Glehen, O., & Degobert, G. (2025). Pulmonary emphysema: Current understanding of disease pathogenesis and therapeutic approaches. Biomedicines, 13(9), 2120. doi:10.3390/biomedicines13092120
D’Cruz, R., Wilkins, D., & Jolley, C. J. (2026). Exercise-induced dynamic hyperinflation in chronic obstructive pulmonary disease. Experimental Physiology. doi:10.1113/EP091459
Downie, P. A. (Ed.). (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Faber and Faber.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for prevention, diagnosis and management of COPD: 2026 report.
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Kwon, C.-Y., Won, J., & Lee, B. (2026). The health effects of diaphragmatic breathing: A systematic review. Complementary Therapies in Medicine, 96, 103317. doi:10.1016/j.ctim.2025.103317
Pereira de Araujo, C. L., Karloh, M., Martins dos Reis, C., Palú, M., & Fleig Mayer, A. (2015). Pursed-lips breathing reduces dynamic hyperinflation induced by activities of daily living test in patients with chronic obstructive pulmonary disease: A randomized cross-over study. Journal of Rehabilitation Medicine, 47(10), 957–962. doi:10.2340/16501977-2008
Rochester, C. L., Alison, J. A., Carlin, B., Jenkins, A. R., Cox, N. S., Bauldoff, G., Bhatt, S. P., Bourbeau, J., Burtin, C., Camp, P. G., Cascino, T. M., Dorney Koppel, G. A., Garvey, C., Goldstein, R., Harris, D., Houchen-Wolloff, L., Limberg, T., Lindenauer, P. K., Moy, M. L., . . . Holland, A. E. (2023). Pulmonary rehabilitation for adults with chronic respiratory disease: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 208(4), e7–e26. doi:10.1164/rccm.202306-1066ST
Sarkar, M., Bhardwaz, R., Madabhavi, I., & Modi, M. (2019). Physical signs in patients with chronic obstructive pulmonary disease. Lung India, 36(1), 38–47. doi:10.4103/lungindia.lungindia_145_18



