
Chronic Bronchitis Airway Clearance: Which Technique Should You Choose?
Compare ACBT, autogenic drainage, PEP and oscillatory PEP for chronic bronchitis, with teaching steps, evidence and a practical decision tree.
Chronic bronchitis is clinically defined as cough with sputum production on most days for at least three months per year for two consecutive years, after excluding other respiratory or cardiac causes.
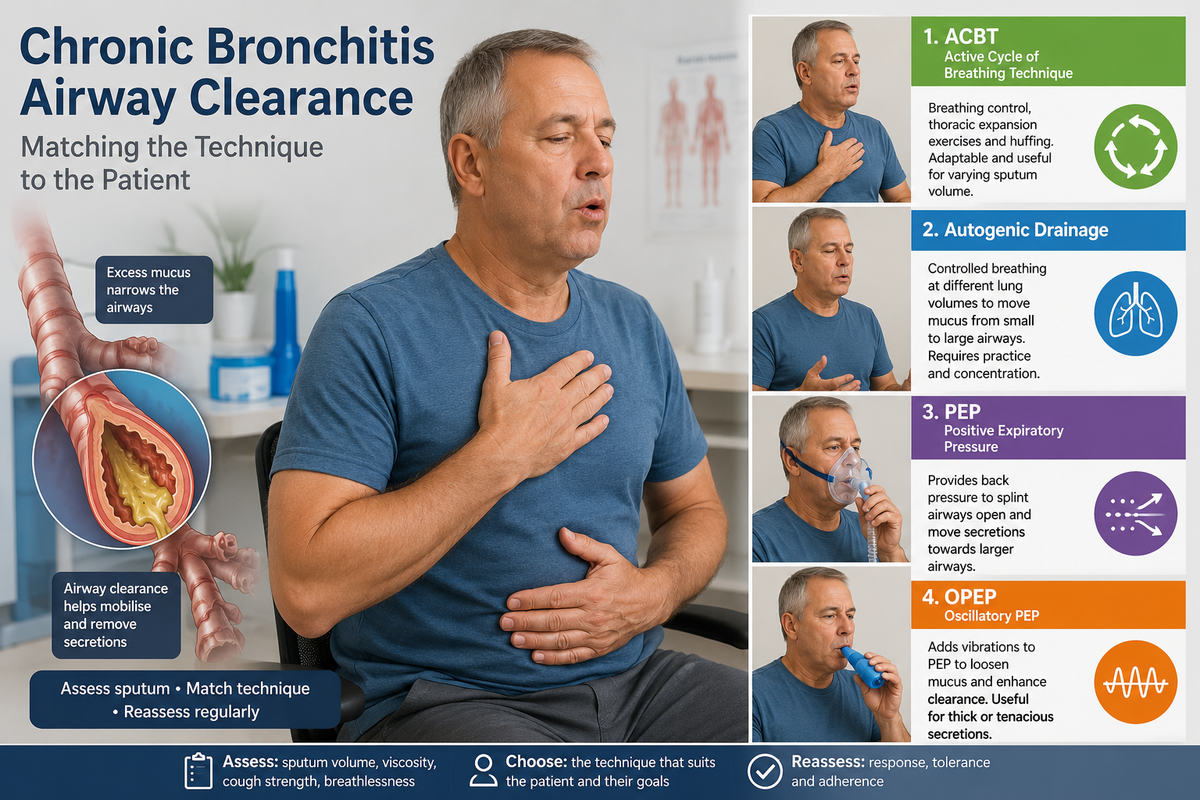
Chronic bronchitis is characterised by persistent productive cough and mucus hypersecretion. Excess mucus narrows already obstructed airways, increases the work of breathing and can contribute to recurrent infection or exacerbation. However, airway-clearance techniques should not be prescribed automatically to every person with COPD. They are most relevant when sputum is present, difficult to expectorate or associated with repeated chest infections. The technique must then be matched to the patient’s respiratory reserve, cognition, coordination and preferences (Lung Foundation Australia, 2025).
Why Sputum Changes the Physiotherapy Plan?
Before choosing a technique, assess sputum volume, colour, viscosity, usual time of production, cough strength, breathlessness, oxygenation and whether bronchiectasis coexists. Also observe whether forceful coughing causes wheezing, airway collapse or marked fatigue. Hydration, prescribed bronchodilation, upright positioning and early mobilisation may improve clearance and should be integrated rather than treating airway clearance as an isolated procedure.
The overall evidence suggests that airway-clearance techniques are generally safe in COPD and may produce modest clinical benefits, but no single method is superior for every patient (Osadnik et al., 2012). More recent guidance similarly favours personalised selection, particularly in patients with mucus hypersecretion. Dyspnoea, contraindications, equipment access and ease of learning all influence the choice (Poncin et al., 2025).
Active Cycle of Breathing Technique: The Practical First Choice
The active cycle of breathing technique, or ACBT, combines breathing control, thoracic expansion exercises and the forced expiratory technique. It is inexpensive, adaptable to different positions and suitable for many patients with mild-to-moderate sputum who can follow a short sequence.
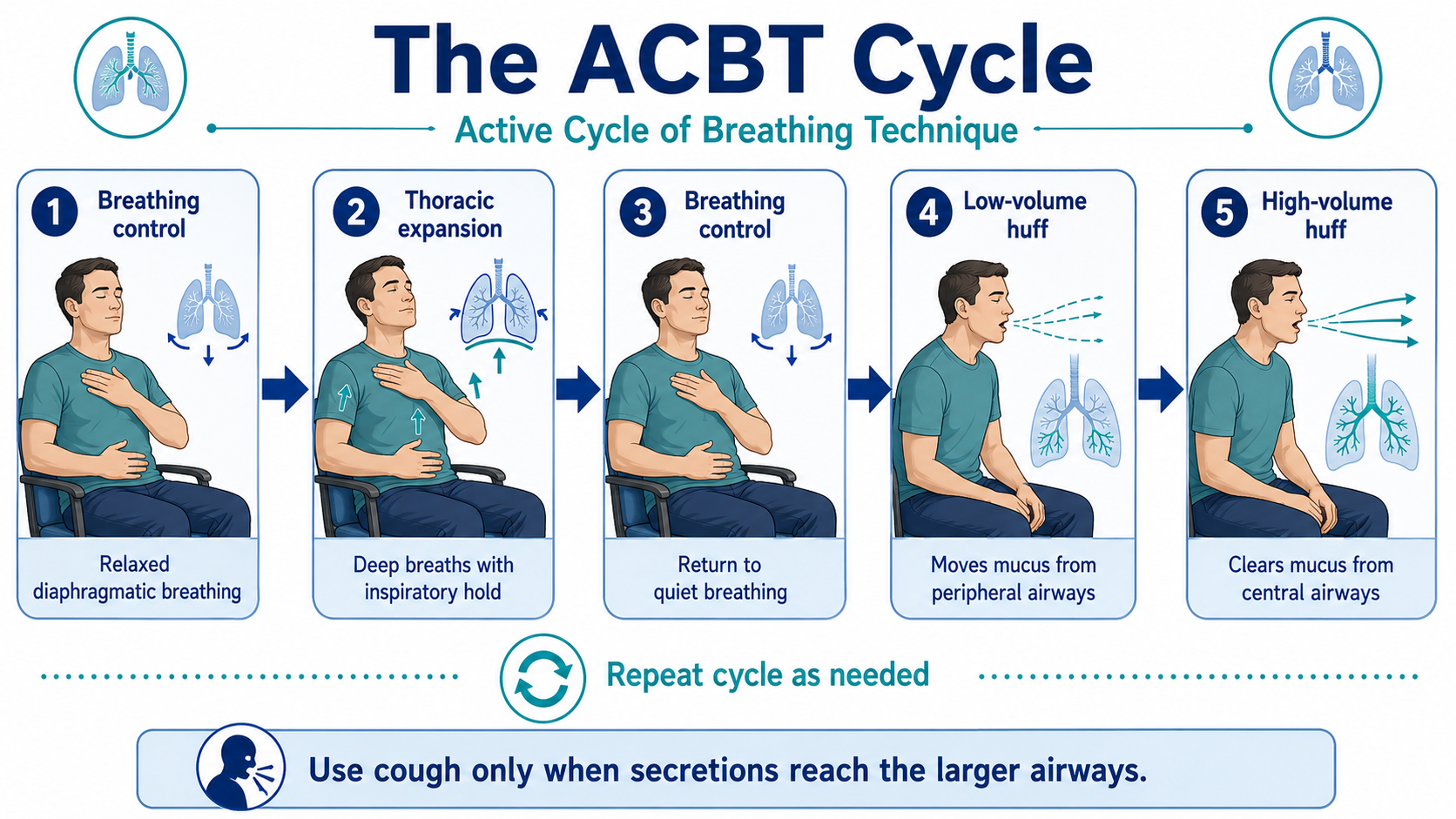
Begin with approximately 20–30 seconds of relaxed breathing control. This is followed by three or four slow thoracic expansion breaths, preferably with a brief inspiratory hold, and then another period of breathing control. The patient performs one or two huffs with the mouth and glottis open. A low-volume huff helps move peripheral secretions, whereas a high-volume huff clears mucus from the larger airways. Coughing is added only when sputum has reached the central airways. The cycle is repeated until the chest feels clearer or the patient begins to fatigue.
ACBT is particularly useful when secretion volume changes from day to day because the cycle can be shortened, lengthened or combined with positioning. Systematic reviews suggest that it improves sputum expectoration and cough efficiency, although improvements in lung function, blood gases and other physiological outcomes are less consistent (Shen et al., 2020; Zisi et al., 2022).
Its main limitation is coordination. A severely breathless, fatigued or cognitively impaired patient may struggle to perform the complete sequence. In such cases, breathing control and huffing can initially be taught as separate components.
Autogenic Drainage: Effective but Skill-Dependent
Autogenic drainage uses controlled breathing at progressively larger lung volumes to move mucus from the smaller to the central airways while limiting premature airway closure. It consists of three phases:
- Unsticking: breathing at low lung volume to mobilise peripheral mucus
- Collecting: breathing at mid-lung volume to gather secretions in medium-sized airways
- Evacuating: breathing at higher lung volume before huffing or coughing
The patient sits comfortably, inhales slowly through the nose, pauses briefly and exhales through an open glottis without forcing the breath. Breathing is repeated at a low lung volume until mucus movement or crackles are felt. The operating lung volume is then gradually increased. A huff or cough is used only when the secretions reach the proximal airways.
Autogenic drainage suits a stable and motivated patient with good concentration, body awareness and control of breathing. It may be useful when repeated forceful coughing produces airway compression, wheezing or excessive fatigue. Sessions generally require 10–20 minutes, and several supervised visits may be needed before the patient can perform the technique independently.
A small randomised study in stable COPD found autogenic drainage broadly comparable with ACBT for secretion clearance and several physiological outcomes (Savci et al., 2000). However, the evidence is limited and relatively old. Autogenic drainage should therefore be selected because it suits the patient—not because it has been proven superior.
Positive Expiratory Pressure: Splinting the Airways Open
Positive expiratory pressure, or PEP, creates resistance during expiration. The resulting back pressure helps stabilise collapsable airways and may promote airflow behind retained mucus, allowing secretions to move towards the larger bronchi. This makes PEP particularly relevant when moderate sputum production is accompanied by dynamic airway compression or an ineffective huff.
Using a mask or mouthpiece, the patient takes a slightly deeper-than-normal breath and exhales actively but not forcefully against the prescribed resistance. A common treatment block consists of 10–15 PEP breaths followed by breathing control and one or two huffs. Several cycles are repeated according to secretion response, breathlessness and fatigue.
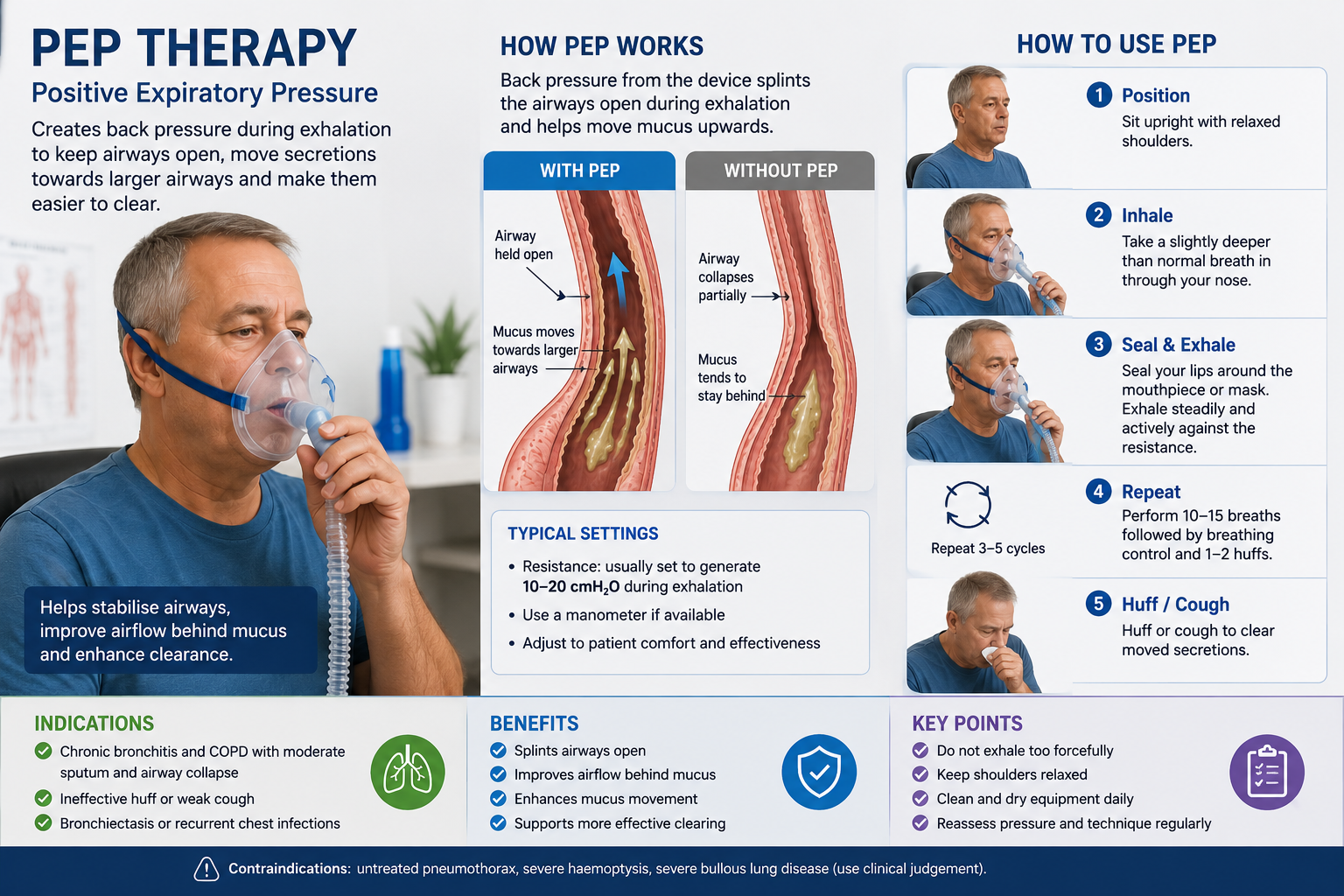
The resistance should be set by a trained clinician rather than selected arbitrarily. It is commonly adjusted to generate approximately 10–20 cmH₂O during expiration while allowing the patient to exhale comfortably.
PEP is easier to standardise than autogenic drainage and can be combined with ACBT. Its limitations include equipment cost, cleaning requirements and the need for an adequate mouthpiece or mask seal. COPD-specific evidence remains less extensive than evidence from cystic fibrosis and bronchiectasis. In acute exacerbations associated with sputum production, PEP-based treatment may reduce hospital stay, but existing studies are not sufficiently conclusive to guarantee this effect (Milan et al., 2019; Osadnik et al., 2012).
Oscillatory PEP: PEP Plus Airway Vibration
Oscillatory positive expiratory pressure, or OPEP, combines expiratory back pressure with vibrations transmitted through the airways. The pressure helps maintain airway patency, while oscillation may reduce mucus adhesiveness and assist its movement towards the mouth. Common devices include Acapella, Flutter and Aerobika, although their mechanisms and position dependence differ.
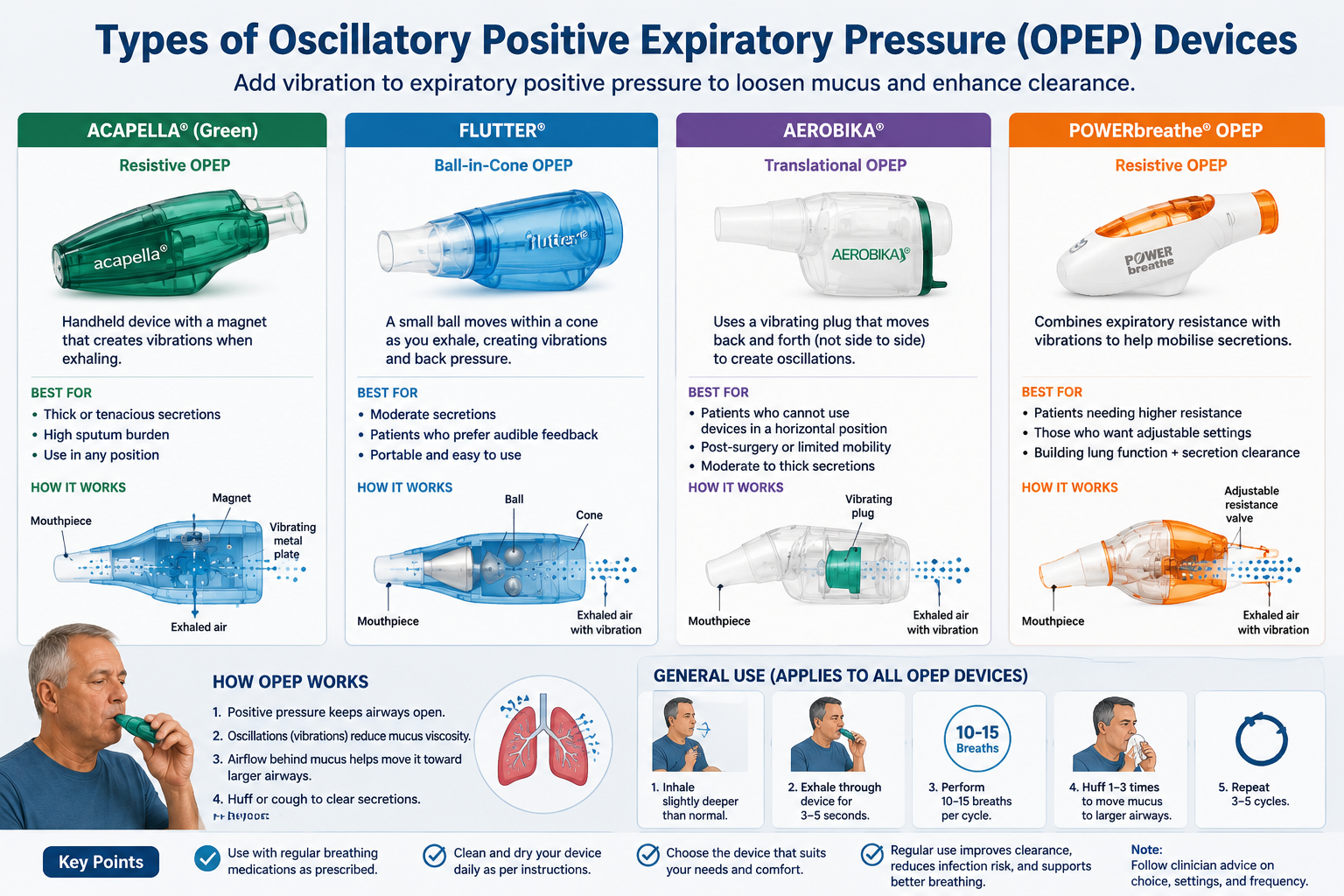
Teach the patient to inhale slightly deeper than tidal volume, hold the breath briefly and exhale steadily through the device for several seconds without completely emptying the lungs. After approximately 10–15 breaths, the patient performs two or three huffs. The cycle is then repeated.
Resistance or device angle should be adjusted until the patient feels a comfortable vibration within the chest rather than only in the mouth. Device-specific cleaning and drying instructions are essential because retained moisture and secretions can contaminate the equipment.
OPEP is particularly appropriate for patients with daily or near-daily sputum, thick secretions and a preference for a portable, independent routine. In a randomised trial involving 122 stable patients with COPD who produced sputum every day or most days, three months of Acapella use improved cough-related quality of life, fatigue, general quality of life and objective cough frequency compared with usual care that included ACBT (Alghamdi et al., 2023).
This provides useful COPD-specific support for OPEP in the chronic sputum-producing phenotype. However, the device should complement rather than replace huffing, exercise, inhaled therapy and appropriate medical management.
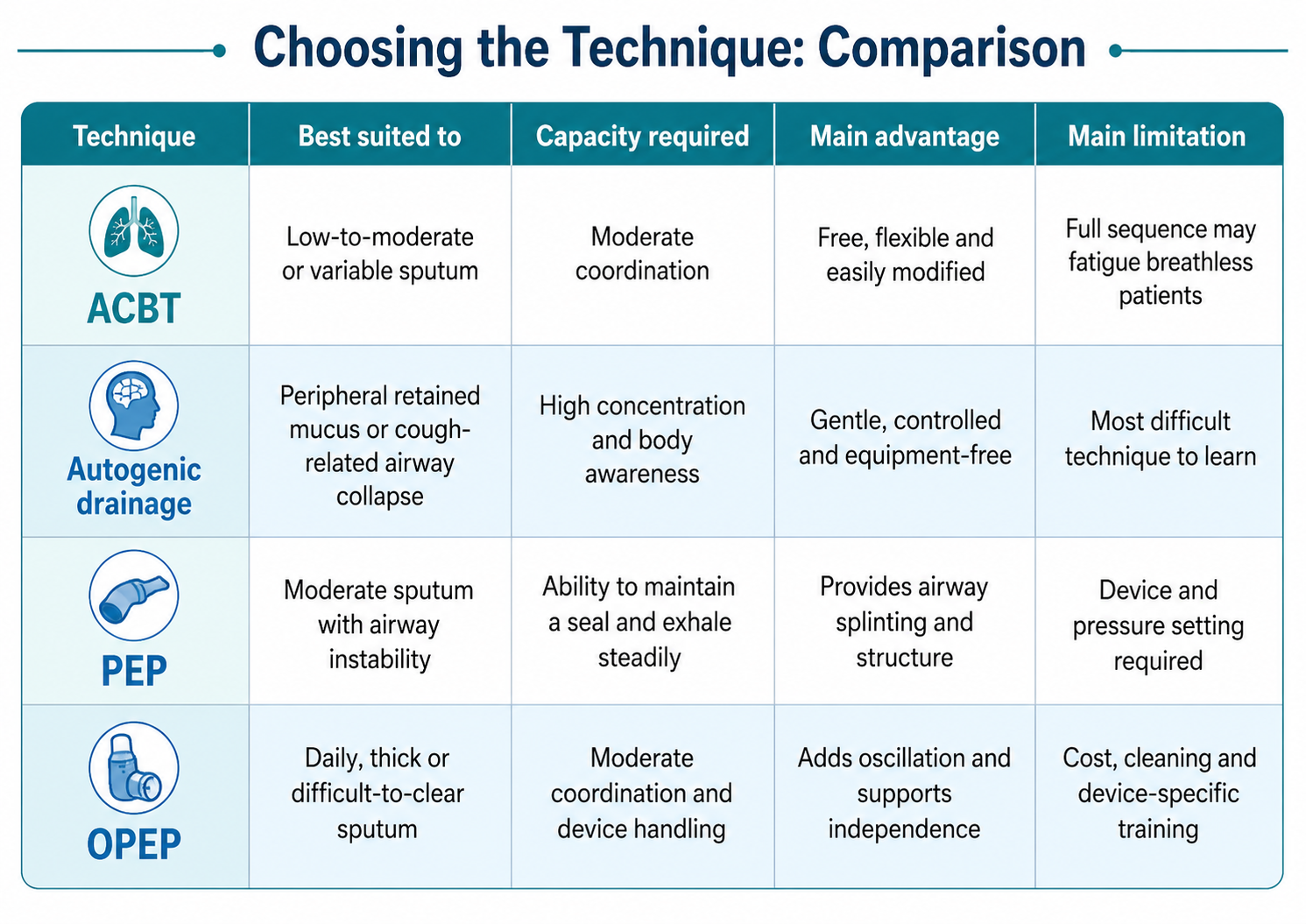
Choosing the Technique: Comparison and Decision Tree
Decision tree
Sputum absent, minimal or cleared easily
→ Routine airway clearance is unlikely to be required. Prioritise exercise, inhaler optimisation, hydration and self-management.
Clinically relevant sputum is present
→ Can the patient understand and coordinate a breathing sequence?
Yes
- Low-to-moderate or variable sputum → Begin with ACBT
- Good body awareness, patience and breath control → Consider autogenic drainage
- Moderate sputum with airway collapse or an ineffective huff → Add PEP
- Daily, thick or high-volume sputum → Consider OPEP followed by huffing or ACBT
No, or the patient is severely fatigued or breathless
→ Use supervised PEP, shortened ACBT components or assisted positioning. Avoid complex autogenic drainage until the patient’s capacity improves.
Treatment should be reassessed using sputum volume, ease of expectoration, breathlessness, oxygen saturation, treatment duration and adherence. The best technique is the one that clears secretions safely and can be performed consistently at home.
Viva-Ready Summary
ACBT is generally the most practical first-line technique because it is flexible, equipment-free and easy to individualise. Autogenic drainage offers controlled clearance with less forceful expiration but demands greater concentration and body awareness. PEP helps splint unstable airways, whereas OPEP adds airway oscillation and currently has the strongest recent COPD-specific evidence for patients with regular sputum production.
Technique selection should be based on sputum burden, airway behaviour, respiratory reserve, cognition and patient preference—not on prescribing habit alone.
One-line recall point: Low or variable sputum favours ACBT: high patient skill favours autogenic drainage; collapsable airways favour PEP; daily tenacious sputum favours OPEP.
References
Alghamdi, S. M., Alsulayyim, A. S., Alasmari, A. M., Philip, K. E. J., Buttery, S. C., Banya, W. A. S., Polkey, M. I., Birring, S. S., & Hopkinson, N. S. (2023). Oscillatory positive expiratory pressure therapy in COPD (O-COPD): A randomised controlled trial. Thorax, 78(2), 136–143.
Downie, P. A. (Ed.). (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Lippincott.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Lung Foundation Australia. (2025). COPD-X Plan: Chest physiotherapy—airway clearance techniques.
Milan, S., Bondalapati, P., Megally, M., Patel, E., Vaghasia, P., Gross, L., Bachman, E. M., Chadha, P., & Weingarten, J. A. (2019). Positive expiratory pressure therapy with and without oscillation and hospital length of stay for acute exacerbation of chronic obstructive pulmonary disease. International Journal of Chronic Obstructive Pulmonary Disease, 14, 2553–2561.
Osadnik, C. R., McDonald, C. F., Jones, A. P., & Holland, A. E. (2012). Airway clearance techniques for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews, 2012(3), CD008328.
Poncin, W., Schrøder, C., Oliveira, A., Herrero-Cortina, B., Cnockaert, P., Gely, L., Osadnik, C., Reychler, G., Mechlenburg, I., & Spinou, A. (2025). Airway clearance techniques for people with acute exacerbation of COPD: A scoping review. European Respiratory Review, 34(175), 240191.
Savci, S., Ince, D. I., & Arikan, H. (2000). A comparison of autogenic drainage and the active cycle of breathing techniques in patients with chronic obstructive pulmonary diseases. Journal of Cardiopulmonary Rehabilitation, 20(1), 37–43.
Shen, M., Li, Y., Ding, X., Xu, L., Li, F., & Lin, H. (2020). Effect of active cycle of breathing techniques in patients with chronic obstructive pulmonary disease: a systematic review of intervention. European Journal of Physical and Rehabilitation Medicine, 56(5), 625–632.
Zisi, D., Chryssanthopoulos, C., Nanas, S., & Philippou, A. (2022). The effectiveness of the active cycle of breathing technique in patients with chronic respiratory diseases: A systematic review. Heart & Lung, 53, 89–98.



