
Bronchiectasis Airway Clearance: Postural Drainage, Modified Positions and Hypertonic Saline
A guide to bronchiectasis physiotherapy covering lobe-specific postural drainage, modified positions for elderly and cardiac patients, the move away from prolonged head-down tilt, and how nebulised hypertonic saline fits into modern airway clearance.
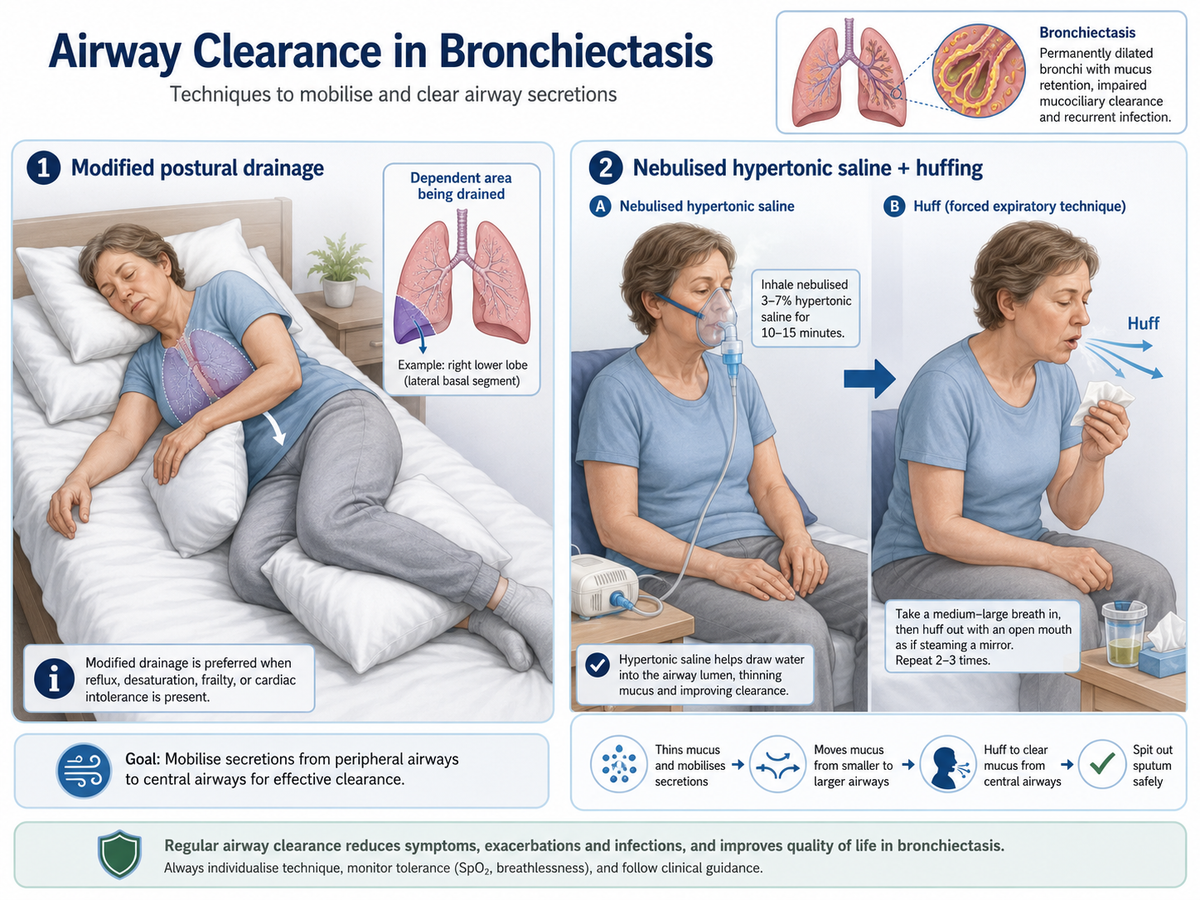
Bronchiectasis is a chronic airway disorder characterised by irreversible bronchial dilatation, chronic sputum production, recurrent infection and impaired mucociliary clearance. For physiotherapists, the practical challenge is simple but important: retained secretions must be mobilised and cleared without worsening breathlessness, reflux, desaturation or cardiovascular strain. That is why modern management no longer treats postural drainage as a rigid routine. Instead, airway-clearance treatment is individualised, segment-targeted and often combined with breathing techniques, huffing, oscillatory devices and, in selected patients, nebulised hypertonic saline (Hill et al., 2019; Polverino et al., 2017).
Why is airway clearance central in bronchiectasis?
Bronchiectasis follows a self-perpetuating cycle of mucus retention, chronic infection, neutrophilic inflammation, airway damage and further mucus retention. When sputum sits in the bronchi, it promotes bacterial colonisation and worsens ventilation, symptoms and exacerbation frequency. Physiotherapy therefore aims to interrupt that cycle by improving secretion transport and reducing air trapping and infection burden (Choi et al., 2024; Polverino et al., 2017).
Airway-clearance sessions are not only about “getting sputum out". They also help reduce work of breathing, improve symptom control and support exercise participation. Commonly used methods include the active cycle of breathing technique (ACBT), autogenic drainage, huffing, postural drainage, positive expiratory pressure (PEP) and oscillatory PEP devices. In practice, postural drainage is often blended with one or more of these rather than used in isolation (Frownfelter & Dean, 2022; O’Neill et al., 2019).
Postural drainage: principle and the shift away from prolonged head-down tilt
Postural drainage uses gravity to assist mucus movement from peripheral to more central airways, from where it can be cleared by huffing or coughing. Classic chest physiotherapy included prolonged head-down positions for middle and lower lobe drainage. However, contemporary practice is more cautious. Many adults with bronchiectasis are older and may also have gastro-oesophageal reflux, obesity, osteoporosis, hypertension, cardiac disease, severe dyspnoea or oxygen desaturation. In such patients, steep Trendelenburg positioning may be poorly tolerated or even inappropriate (Hill et al., 2019; O’Neill et al., 2019).
This has led to a shift toward modified postural drainage, where the therapist preserves the direction of drainage but reduces or removes the head-down angle. The patient may be positioned flat, side-lying, semi-reclined or supported with pillows. This is especially useful for elderly, frail and cardiac patients. The clinical message is not that gravity is unimportant; rather, it is that tolerability and safety often determine the best position (Frownfelter & Dean, 2022; Hillegass, 2016).
Situations where prolonged head-down tilt is commonly avoided or modified include:
- symptomatic reflux or aspiration risk
- unstable cardiovascular status, arrhythmia or orthopnoea
- uncontrolled hypertension
- severe breathlessness or desaturation in the position
- recent haemoptysis
- raised intracranial pressure or recent neurosurgery
- late pregnancy or marked obesity
- immediately after meals
Lobe-specific postural drainage positions
The affected lobe or segment should ideally be identified from imaging, auscultation and the patient’s sputum pattern. In diffuse bilateral disease, the therapist prioritises the most symptomatic or most secretion-laden regions.
Table 1
Common lobe-specific drainage positions and practical modifications


These positions are usually paired with thoracic expansion exercises, breathing control, huffs and coughs. Segmental percussion and vibrations may still be used selectively, although many modern programmes rely more on breathing-based clearance and self-management techniques than on passive manual techniques alone (Cash/Downie, 1993; Frownfelter & Dean, 2022).
Modified positions for elderly and cardiac patients
Elderly patients and those with cardiac comorbidity often need drainage that is effective yet haemodynamically lighter. A useful principle is: drain first, strain less.
Practical adaptations include using:
- high side-lying instead of steep head-down side-lying
- semi-reclined or flat positions instead of Trendelenburg
- shorter position holds with rest breaks
- pillow support under the trunk, hips or shoulders
- ACBT or huffing in upright sitting after each position change
- pulse, SpO₂ and symptom monitoring during treatment
For a patient with heart failure, orthopnoea or postoperative cardiac limitations, lying flat or head-down may worsen distress. In such cases, supported sitting, side-lying and upright clearance with PEP/OPEP may be more realistic. Similarly, in frail older adults, the “best” position is not the most dramatic angle but the one the patient can repeat safely and independently at home (Hill et al., 2019; Hillegass, 2016).
Nebulised hypertonic saline and its role with physiotherapy
Nebulised hypertonic saline is a useful adjunct in selected patients with tenacious sputum. Its rationale is osmotic: it draws water into the airway surface liquid, improves mucus hydration and can make sputum easier to expectorate. In bronchiectasis, guidelines suggest considering long-term mucoactive treatment in patients who have difficulty clearing sputum and poor quality of life despite standard airway-clearance techniques; recombinant human DNase, however, is not recommended in non-CF bronchiectasis (Polverino et al., 2017).
Evidence for hypertonic saline is supportive but not uniform. Trials using 6%–7% solutions have shown improved sputum clearance and, in some studies, gains in lung function, quality of life or healthcare use, although results across studies are mixed and not all patients benefit equally (Kellett & Robert, 2011; Nicolson et al., 2012; O’Neill et al., 2019). That is why hypertonic saline should be seen as an adjunct, not a replacement for physiotherapy.
A practical sequence is the following:
- Bronchodilator first if there is bronchial hyperreactivity or prior bronchospasm risk.
- Nebulised hypertonic saline under appropriate monitoring or after an initial tolerance test.
- Airway-clearance technique such as ACBT, postural drainage, ELTGOL, PEP or OPEP.
- Huff and cough to complete sputum evacuation.
Important precautions include cough irritation, throat irritation, bronchospasm and transient desaturation. Many centres perform an initial supervised trial and avoid routine use if the patient cannot tolerate it. In simple language: hypertonic saline helps loosen sputum, but the sputum still needs physiotherapy to come out.
Putting it together: a modern physiotherapy session
A typical modern session for bronchiectasis may include assessment of sputum load, breathlessness, oxygenation, reflux history and the distribution of disease; selection of one or two relevant drainage positions; incorporation of ACBT or huffing; and choice of adjuncts such as OPEP or hypertonic saline when indicated. Treatment is then progressed into exercise and self-management, because regular physical activity and pulmonary rehabilitation are also important parts of long-term care (Polverino et al., 2017).

The strongest clinical takeaway is that postural drainage has evolved. It is no longer a one-size-fits-all, prolonged head-down routine. It is now a targeted, patient-centred component of an airway-clearance programme.
Viva-Ready Summary
Bronchiectasis causes chronic sputum retention because damaged airways and impaired mucociliary clearance promote mucus stasis. Physiotherapy remains a cornerstone of management. Postural drainage helps use gravity to mobilise secretions from affected lobes, but modern practice individualises the angle and duration of positioning. Prolonged head-down tilt is used less often because many patients cannot tolerate it and because modified positions can often achieve secretion clearance more safely. Elderly and cardiac patients usually do better with flat, side-lying or semi-reclined modified drainage combined with ACBT, huffing and sometimes PEP/OPEP. Nebulised hypertonic saline is an adjunct for selected patients with thick sputum, especially when used before airway-clearance physiotherapy, but it requires tolerance assessment and does not replace the clearance technique itself.
One-line recall point:
In bronchiectasis, modern airway clearance means “the right technique, in the right position, for the right patient".
References
Choi, H., Yang, B., & Chalmers, J. D. (2024). Bronchiectasis management in adults: State of the art and future directions. European Respiratory Journal, 63(6), 2400518. https://doi.org/10.1183/13993003.00518-2024
Downie, P. A. (Ed.). (1993). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Jaypee Brothers Medical Publishers.
Frownfelter, D., & Dean, E. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
Hillegass, E. (2016). Essentials of cardiopulmonary physical therapy (4th ed.). Elsevier.
Hill, A. T., Sullivan, A. L., Chalmers, J. D., De Soyza, A., Elborn, J. S., Floto, R. A., Grillo, L., Gruffydd-Jones, K., Harvey, A., Haworth, C. S., Loebinger, M. R., Milross, M., Nightingale, M., O’Donnell, A., Panko, M., Prasad, A., Smith, M. P., Tunney, M., Whitters, D., … Wilson, R. (2019). British Thoracic Society guideline for bronchiectasis in adults. Thorax, 74(Suppl 1), 1–69. https://doi.org/10.1136/thoraxjnl-2018-212463
Kellett, F., & Robert, N. M. (2011). Nebulised 7% hypertonic saline improves lung function and quality of life in bronchiectasis. Respiratory Medicine, 105(12), 1831–1835. https://doi.org/10.1016/j.rmed.2011.07.019
Nicolson, C. H. H., Stirling, R. G., Borg, B. M., Button, B. M., Wilson, J. W., & Holland, A. E. (2012). The long-term effect of inhaled hypertonic saline 6% in non-cystic fibrosis bronchiectasis. Respiratory Medicine, 106(5), 661–667. https://doi.org/10.1016/j.rmed.2012.01.021
O’Neill, K., O’Donnell, A. E., & Bradley, J. M. (2019). Airway clearance, mucoactive therapies and pulmonary rehabilitation in bronchiectasis. Respirology, 24(3), 227–237. https://doi.org/10.1111/resp.13459
Polverino, E., Goeminne, P. C., McDonnell, M. J., Aliberti, S., Marshall, S. E., Loebinger, M. R., Murris, M., Cantón, R., Torres, A., Dimakou, K., De Soyza, A., Hill, A. T., Haworth, C. S., Vendrell, M., Ringshausen, F. C., Subotic, D., Wilson, R., Vilaró, J., Stallberg, B., … Chalmers, J. D. (2017). European Respiratory Society guidelines for the management of adult bronchiectasis. European Respiratory Journal, 50(3), 1700629. https://doi.org/10.1183/13993003.00629-2017
Lee, A. L., Burge, A. T., & Holland, A. E. (2015). Airway clearance techniques for bronchiectasis. Cochrane Database of Systematic Reviews, (11), CD008351. https://doi.org/10.1002/14651858.CD008351.pub3



