
Before the Bypass: The Complete Pre-CABG Physiotherapy Protocol
Learn the complete pre-CABG physiotherapy protocol, including respiratory assessment, 6MWT, IMT, incentive spirometry, cough training and viva points.
Coronary artery bypass grafting (CABG) restores myocardial blood flow, but the operation temporarily challenges the respiratory system. General anaesthesia, median sternotomy, cardiopulmonary bypass, pain, pleural drains and postoperative immobility can reduce lung volumes, weaken cough and promote secretion retention or atelectasis. Pre-CABG physiotherapy therefore begins before the incision: it identifies risk, builds respiratory reserve and rehearses the skills the patient will need immediately after extubation (Frownfelter et al., 2022).
Why Does Physiotherapy Start Before CABG?
The aim of preoperative physiotherapy is not to “make the lungs perfect” in a few days. It is to reduce avoidable risk and make postoperative care familiar. A patient who has already practised deep breathing, supported coughing and bed mobility is more likely to perform these techniques correctly despite pain, anxiety and fatigue.
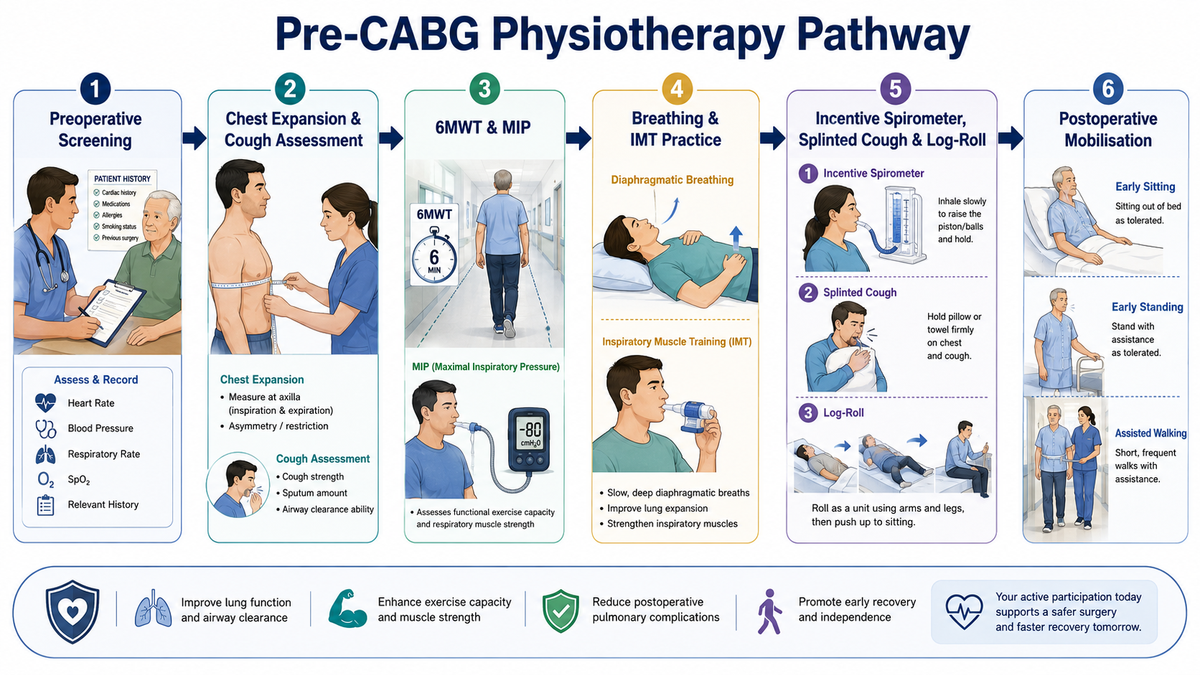
The physiotherapist has three core responsibilities:
- Assess: Establish respiratory and functional baselines and identify patients at increased risk of postoperative pulmonary complications (PPCs).
- Prepare: Prescribe suitable breathing exercises, inspiratory muscle training (IMT) or general activity when indicated.
- Educate: Teach incentive spirometry, splinted cough, log-rolling and the expected progression to sitting, standing and walking.
This assessment should be coordinated with the surgical and anaesthesia teams. Exercise testing or training is inappropriate when the patient has unstable angina, uncontrolled arrhythmia, decompensated heart failure, acute infection or another contraindication to exertion.
Preoperative Assessment: What Should Be Documented?
Begin with the medical record and a focused interview. Note the planned procedure, urgency of surgery, left ventricular function, recent myocardial infarction or angina, smoking history, diabetes, obesity, chronic respiratory disease, previous thoracic surgery, mobility level and home support. Ask about dyspnoea, orthopnoea, cough, sputum, fatigue and the activities that currently provoke symptoms.
The physical assessment should include:
| Domain | What to assess | Why it matters |
|---|---|---|
| Baseline observations | Heart rate, blood pressure, respiratory rate, SpO₂, pain and symptoms | Establishes safety and allows postoperative comparison |
| Breathing pattern | Rate, depth, accessory-muscle use, symmetry and diaphragmatic movement | Detects inefficient or shallow breathing |
| Chest expansion | Tape measurement at consistent anatomical levels, commonly axillary and xiphisternal | Provides a simple baseline of thoracic excursion |
| Auscultation | Air entry and added sounds | Identifies secretion load, reduced ventilation or coexisting pathology |
| Cough | Voluntary cough strength, pain, sputum and ability to huff | Predicts the ability to clear secretions after surgery |
| Functional capacity | Baseline six-minute walk test, when medically stable | Quantifies submaximal exercise capacity and symptoms |
| Inspiratory muscles | Maximal inspiratory pressure, when equipment is available | Screens for inspiratory muscle weakness and helps prescribe IMT |
| Frailty and mobility | Gait, transfers, sit-to-stand or handgrip strength | Anticipates postoperative assistance and discharge needs |
For the six-minute walk test (6MWT), record distance, pre- and post-test heart rate, blood pressure, SpO₂, Borg dyspnoea and perceived exertion. Standardised instructions and encouragement improve reproducibility (Holland et al., 2014). Stop the test if the patient develops chest pain, marked dizziness, pallor, staggering, intolerable dyspnoea or another concerning clinical response.
IMT screening is preferably performed by measuring maximal inspiratory pressure, also written as MIP or PImax. Inspiratory muscle training (IMT) screening is the preoperative assessment of inspiratory muscle strength to identify patients who may benefit from targeted breathing-muscle training before CABG. It is commonly performed by measuring maximal inspiratory pressure (MIP or PImax) using a handheld respiratory pressure device. The patient exhales fully and then inhales as forcefully as possible against an occluded mouthpiece. A low value, interpreted against age- and sex-based reference values, may indicate inspiratory muscle weakness.
Breathing Preparation and Prehabilitation Protocol
Every patient does not require the same programme. The intervention should match the time available, clinical stability and identified impairments.
1. Breathing control and thoracic expansion
Teach relaxed diaphragmatic breathing followed by slow, deep inspirations. A brief inspiratory hold may assist ventilation to slower-filling lung regions, after which the patient exhales gently. Avoid rapid, repeated maximal breaths that produce dizziness.
2. Huffing and coughing
Practise one or two huffs from medium-to-high lung volume, followed by a cough when secretions are present. Correct technique is more valuable than repeated forceful coughing.
3. Inspiratory muscle training
For stable, higher-risk elective patients, threshold IMT may begin at approximately 30% of measured MIP and be progressed according to symptoms, perceived effort and repeat measurements. The landmark CABG trial used 20 minutes of training daily for at least two weeks, with weekly physiotherapist supervision, and reduced PPCs (Postoperative Pulmonary Complications) in high-risk patients (Hulzebos et al., 2006). This provides a research-informed starting framework, not an automatic prescription for every patient.
4. General physical preparation
When cleared by the cardiology team, encourage symptom-limited walking, functional strengthening and avoidance of prolonged inactivity. Training intensity should remain below the level that provokes angina, abnormal haemodynamic responses or excessive breathlessness.
5. Risk modification and planning
Reinforce smoking cessation, medication adherence, nutrition, glucose control and treatment of active respiratory infection through the appropriate medical team. Discuss anticipated mobility aids, family assistance and potential discharge barriers. Contemporary cardiac surgery practice increasingly combines physical assessment with frailty screening and prehabilitation planning (Society of Thoracic Surgeons, 2026).
Does Prehabilitation Reduce Pulmonary Complications?
The strongest classic evidence supports targeted inspiratory training in higher-risk patients. Hulzebos et al. (2006) reported PPCs in 18% of the preoperative IMT group compared with 35% of the usual-care group. Pneumonia was also less frequent, and the median postoperative stay was shorter.
Evidence for incentive spirometry is more nuanced. A 2021 CABG trial found less atelectasis and shorter ventilation and hospital stay when preoperative incentive spirometry was combined with deep breathing, coughing and postoperative early ambulation (Sweity et al., 2021). However, incentive spirometry should not be presented as a stand-alone protective device.
The American Association for Respiratory Care recommends combining incentive spirometry with deep breathing, directed coughing, early mobilisation and adequate analgesia. It advises against the routine use of incentive spirometry alone to prevent atelectasis after CABG (Restrepo et al., 2011).
In the 2023 PREPs trial, combined exercise and IMT were safe but did not outperform standard care for improvement in preoperative 6MWT distance across an unselected elective cardiac-surgery group (Akowuah et al., 2023). The practical conclusion is that prehabilitation is most defensible when it is risk-stratified, supervised and impairment-directed, rather than applied identically to every CABG patient.
Preoperative Patient Education: Rehearsing Postoperative Recovery
Preoperative education helps patients practise essential postoperative techniques while they are comfortable, alert and less anxious. After CABG, pain, anaesthesia and reduced mobility may lead to shallow breathing, secretion retention and fear of movement. The physiotherapist should therefore explain the importance of lung expansion, effective coughing and early mobilisation before surgery.
Incentive Spirometry
The patient should sit upright, breathe out normally and then inhale slowly and deeply through the mouthpiece. The breath is held briefly before relaxed exhalation. Normal breaths should be taken between attempts to prevent dizziness or fatigue.
The patient must understand that the device is used by inhaling, not blowing into it. The aim is a slow, sustained inspiration rather than rapidly raising the indicator or chasing a high numerical value. Incentive spirometry should be combined with deep breathing, coughing, pain control and early mobilisation.

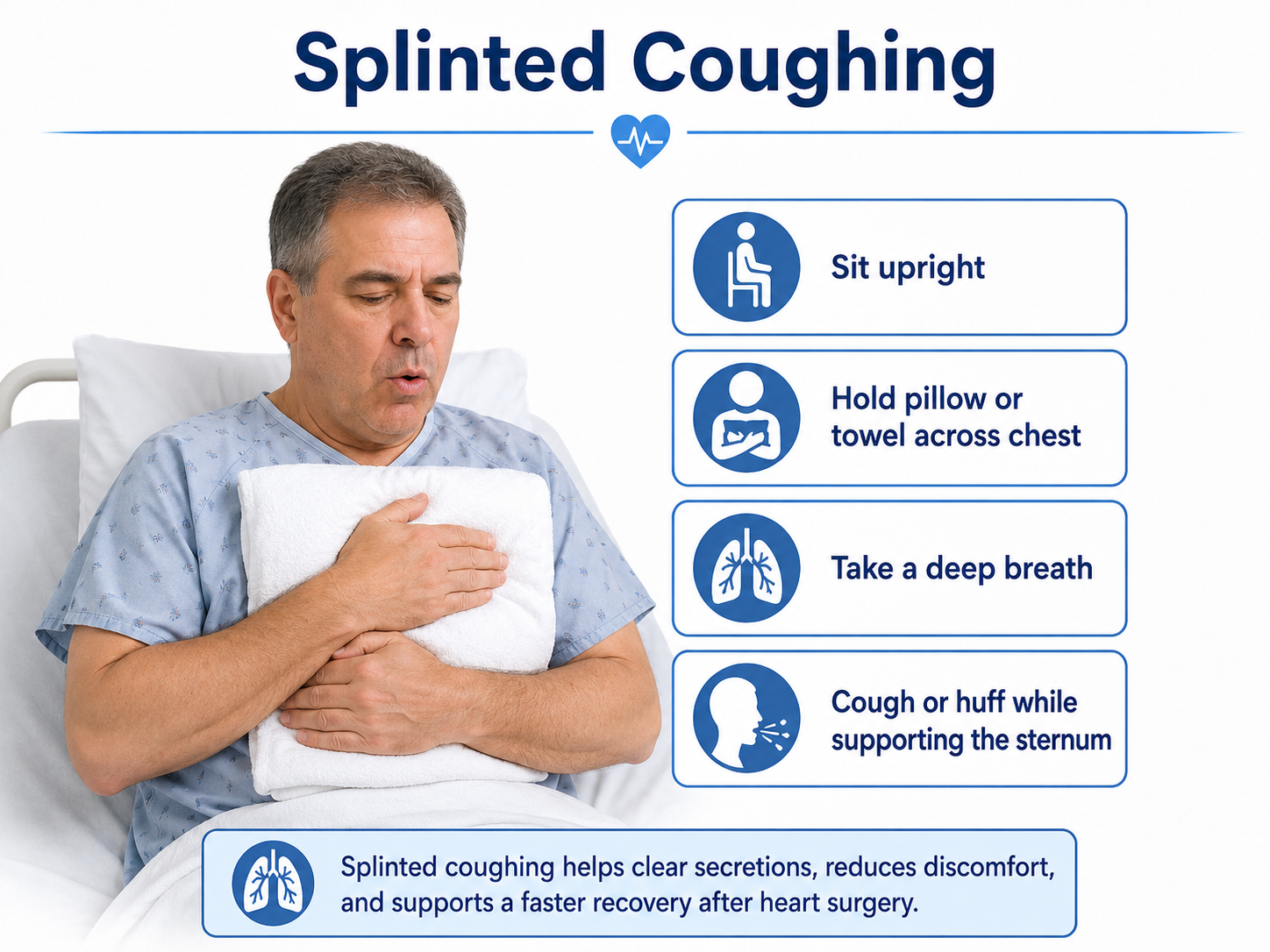
Splinted Coughing
Pain or fear of stressing the sternotomy may cause patients to suppress coughing, increasing the risk of secretion retention. During a splinted cough, the patient supports the chest with a folded towel, pillow or approved device, takes a deep breath and performs one or two huffs or coughs.
Splinting may improve comfort and confidence but does not replace adequate analgesia. Pain that prevents effective breathing or coughing should be reported to the medical or nursing team.
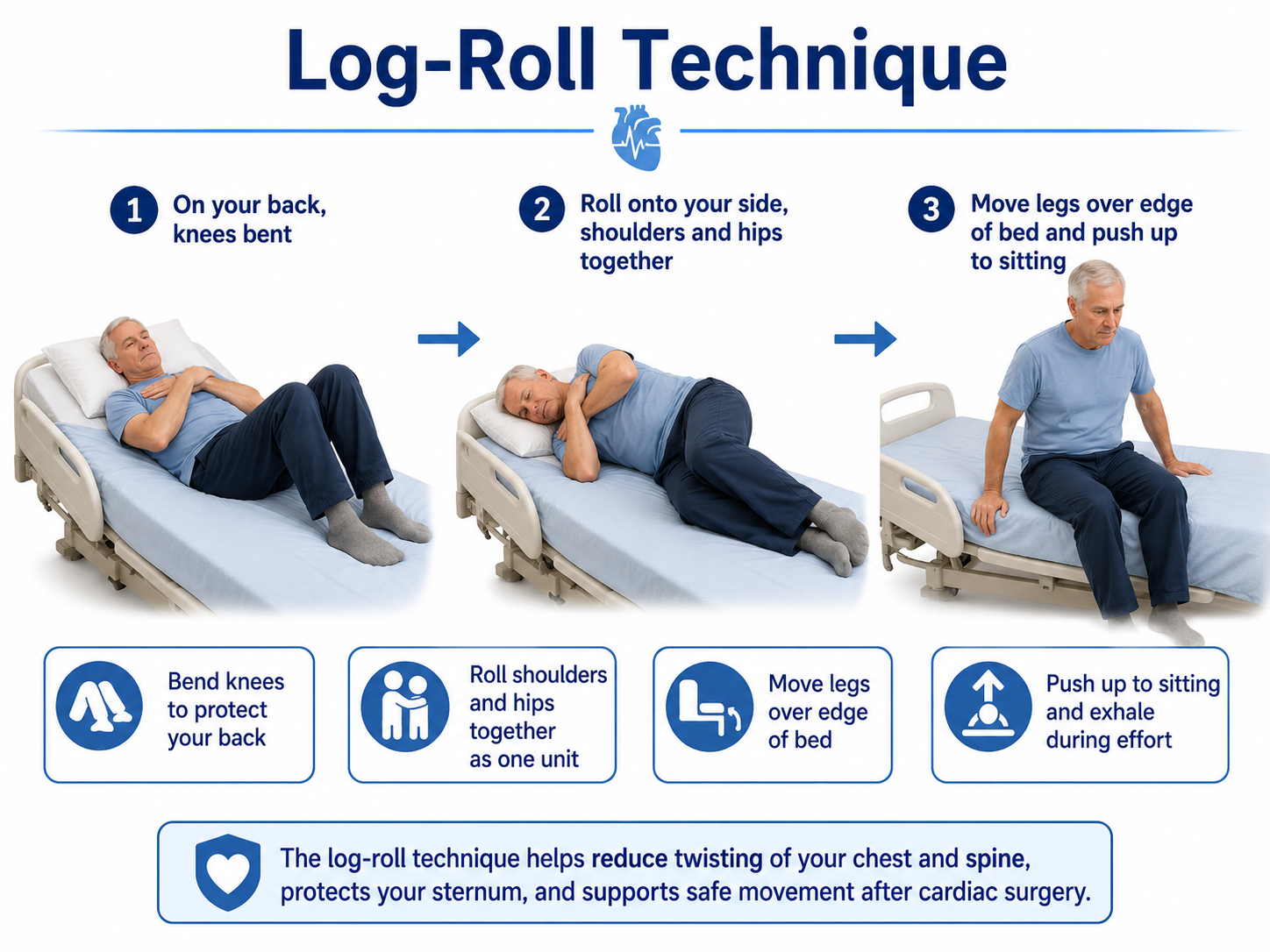
Log-Roll Technique
The log-roll technique helps the patient move from lying to sitting while limiting excessive trunk rotation. The knees are bent, and the shoulders, trunk and pelvis are rolled together onto one side. The legs are then moved over the edge of the bed as the patient pushes into sitting.
The patient should exhale during effort and avoid forcefully pulling on bedrails, walkers or another person. Upper-limb use should follow the surgeon’s or institution’s sternal-movement guidance.
Confirming Understanding
The session should end with supervised return demonstration of incentive spirometry, splinted coughing and log-rolling. This allows the physiotherapist to correct errors and confirm that the patient understands both the technique and its purpose.
Viva-Ready Summary: What the Examiner Expects
A strong viva answer should follow a logical sequence:
“Pre-CABG physiotherapy includes risk assessment, baseline respiratory and functional evaluation, targeted prehabilitation and postoperative education. I assess vital signs, breathing pattern, chest expansion, auscultation, cough and sputum, baseline 6MWT in stable patients, and MIP for inspiratory muscle weakness. Intervention includes breathing exercises, huffing and supported cough, selective IMT, safe activity and risk-factor education. I teach incentive spirometry as part of a bundle—not alone—together with splinted coughing, log-rolling, pain control and early mobilisation. The goal is to reduce pulmonary-complication risk, improve readiness and establish baselines for postoperative rehabilitation.”
One-line viva recall
Assess the risk, train the breath, and rehearse the recovery.
References
Akowuah, E. F., Wagnild, J. M., Bardgett, M., Prichard, J. G., Mathias, A., Harrison, S. L., Ogundimu, E. O., Hancock, H. C., Maier, R. H., & PREPs Trial Investigators. (2023). A randomised controlled trial of prehabilitation in patients undergoing elective cardiac surgery. Anaesthesia, 78(9), 1120–1128. https://doi.org/10.1111/anae.16072
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Mosby.
Holland, A. E., Spruit, M. A., Troosters, T., Puhan, M. A., Pepin, V., Saey, D., McCormack, M. C., Carlin, B. W., Sciurba, F. C., Pitta, F., Wanger, J., MacIntyre, N., Kaminsky, D. A., Culver, B. H., Revill, S. M., Hernandes, N. A., Andrianopoulos, V., Camillo, C. A., Mitchell, K. E., . . . Singh, S. J. (2014). An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. European Respiratory Journal, 44(6), 1428–1446. https://doi.org/10.1183/09031936.00150314
Hulzebos, E. H. J., Helders, P. J. M., Favié, N. J., De Bie, R. A., Brutel de la Rivière, A., & Van Meeteren, N. L. U. (2006). Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: A randomized clinical trial. JAMA, 296(15), 1851–1857. https://doi.org/10.1001/jama.296.15.1851
Restrepo, R. D., Wettstein, R., Wittnebel, L., & Tracy, M. (2011). Incentive spirometry: 2011. Respiratory Care, 56(10), 1600–1604. https://doi.org/10.4187/respcare.01471
Society of Thoracic Surgeons. (2026). Prehab power: Enhancing surgical success through frailty assessment and prehabilitation [Webinar slides].
Sweity, E. M., Alkaissi, A. A., Othman, W., & Salahat, A. (2021). Preoperative incentive spirometry for preventing postoperative pulmonary complications in patients undergoing coronary artery bypass graft surgery: A prospective, randomized controlled trial. Journal of Cardiothoracic Surgery, 16, Article 241. https://doi.org/10.1186/s13019-021-01628-2



